GRID VIEW

I remember my introduction to puberty, my real introduction. It wasn’t a growth spurt, a voice change, or new body hair. It was a big. fat. zit. Right on the face. I was lucky, only getting a few zits here and there, but they still managed to kill my confidence. Unfortunately, it can be much, much worse for many people. Acne affects hundreds of millions of people worldwide and millions in the United States alone. Though most (85%) people experience acne in adolescence, nearly half of adults in their twenties have the condition. Beyond a simple zit here or there, acne can cause grease, lesions, and permanent scarring to the face and upper body. Acne can be graded based on the severity as mild, moderate, or severe. This can have serious negative impacts on mental health and quality of life. To really get under the skin of what’s going on with acne and what to do about it we first have to understand where and how it happens. Acne arises in the sebaceous gland. Sebaceous comes from Latin and shares its root word with soap. These glands produce an oily fat called sebum that coats our hair and skin and helps keep them from drying out. Instead of being gross, they are super helpful. The gland itself is embedded in the skin with a hair follicle, where hair is made. Together, these make up a pilosebaceous unit (Latin for hair-grease). Along with producing oils, the sebaceous gland also has the ability to sense its surroundings. It detects and responds to changes on the skin and hormonal changes in the body. Unfortunately, they can be confused and cause acne.
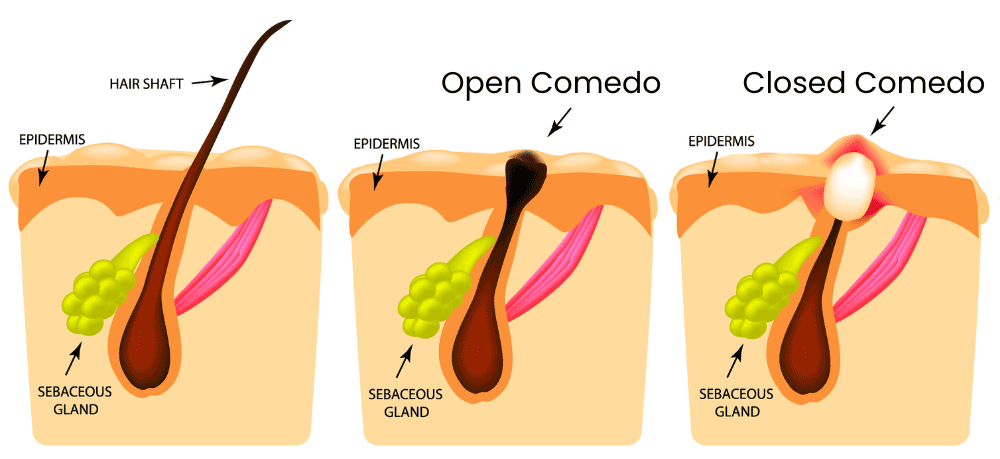
There are many causes of acne, but they can be roughly divided into four main factors: increased sebum, obstruction of the pilosebaceous unit, colonization by a bacterium, and an inflammatory response. Increased sebum is when too much of the oily, waxy fat is produced. This is usually called androgen-mediated sebogenesis, which gives a clue. The issue is an imbalance of hormones known as androgens. These are a type of steroid that can cause the sebaceous gland to produce too much sebum, which can clog the pilosebaceous unit. This brings us to obstruction of the pilosebaceous unit. Most of the machinery of the pilosebaceous unit is located in the middle layer of skin, and it squeezes out of a small pore at the top. This pore can get clogged by sebum and hair components. A small clog is called a microcomedo. The micro– is there because the skin still looks and feels normal. If the buildup continues, there is swelling and we get a full comedo (plural comedones). This is the zit, a clogged pilosebaceous unit. Side note: the comedo can be fully covered (closed) or exposed to air (open). When covered, skin pigments are preserved and we get a whitehead. When open, oxygen causes discoloration and darkening of the sebum, leading to a blackhead. But why does the buildup start? What’s causing this excess production? Surprisingly, the culprit has to do with the skin microbiome! This includes large amounts of (mostly helpful) bacteria that live on and in the top few layers of the skin. With acne, the little guy in question is named cutibacterium acnes, formerly called propionibacterium acnes. This bacteria is everywhere and lives happily without oxygen inside your pilosebaceous unit your whole life. It usually regulates the stability of the sebaceous gland. There are multiple strains of cutibacterium acnes (c. acnes), and some are worse than others. On the surfaces of the bacteria are proteins that vary by strain and conditions around the sebaceous gland. These can help it survive and can fight other bacteria. In some instances, these proteins can attach to the parts of the pilosebaceous unit that sense its environment. In acne-causing strains of c. acnes, the proteins activate receptors that regulate inflammatory responses. These strains are more likely to be dominant when the skin microbiome is out of whack and/or the pilosebaceous unit is producing too much sebum. The problem with c. acnes, then, isn’t the bacteria itself, but destructive strains and a skewed skin microbiome. This brings us to the last factor contributing to acne: inflammation. Inflammation is the body’s response to dangerous invaders. It is responsive and quick but can have trouble learning from its mistakes. With acne, the inflammation system is activated by rogue c. acnes strains and attacks enemies that aren’t there. This results in the reddening and swelling typical of a zit. So, what can be done about acne? With the enormous number of people who get acne and the very public nature, there are a lot of treatments with varying results. Skin cleansers have inconsistent data showing efficacy. The first medical lines of defense are topical agents. Retinoids, derived from vitamin A, bind to skin cells and promote extra skin cell production, which helps clear sebaceous ducts and microcomedones. Benzoyl peroxide is cheap and effective, generating killer free radicals that enter the pilosebaceous unit and kill c. acnes indiscriminately. Topical antibiotics can be effective at combating rogue c. acnes, but improper or excessive use can create antibiotic resistance, an increasing problem with acne. The second lines of defense are systemic agents that affect the whole body. These include medications that suppress androgens, oral antibiotics, and systemic retinoids. Since they are systemic, side effects are typically more severe than with topical treatments, but they can be used to treat moderate-to-severe acne. But what if there were another way? On the very verge of research is a c. acnes vaccine! An effective vaccine would target just the dangerous strains of the bacteria and would hopefully provide lasting protection. With luck, future generations can be introduced to puberty with parental embarrassment instead of acne! Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Barbieri, J. S., Wanat, K., & Seykora, J. (2014). Skin: basic structure and function. https://www.sciencedirect.com/referencework/9780123864574/pathobiology-of-human-disease Das, S., & Reynolds, R. V. (2014). Recent advances in acne pathogenesis: implications for therapy. American journal of clinical dermatology, 15, 479-488. https://link.springer.com/article/10.1007/s40257-014-0099-z Del Rosso, J. Q., & Kircik, L. (2024). The cutaneous effects of androgens and androgen-mediated sebum production and their pathophysiologic and therapeutic importance in acne vulgaris. Journal of Dermatological Treatment, 35(1), 2298878. https://www.tandfonline.com/doi/full/10.1080/09546634.2023.2298878 Dréno, B., Pécastaings, S., Corvec, S., Veraldi, S., Khammari, A., & Roques, C. (2018). Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates. Journal of the European Academy of Dermatology and Venereology, 32, 5-14. https://doi.org/10.1111/jdv.15043 Mayslich, C., Grange, P. A., Castela, M., Marcelin, A. G., Calvez, V., & Dupin, N. (2022). Characterization of a Cutibacterium acnes Camp Factor 1-Related Peptide as a New TLR-2 Modulator in In Vitro and Ex Vivo Models of Inflammation. International Journal of Molecular Sciences, 23(9), 5065. https://doi.org/10.3390%2Fijms23095065 Mayslich, C., Grange, P. A., & Dupin, N. (2021). Cutibacterium acnes as an opportunistic pathogen: An update of its virulence-associated factors. Microorganisms, 9(2), 303.
Listen to the article here:

According to current studies, more than 8 million Americans suffer from psoriasis, but what is it really? By definition, psoriasis is a condition that causes skin cells to multiply rapidly, and consequently build-up on the surface of the skin. This can cause scaly, red patches that are often itchy, painful, and sore. While the exact cause is unclear, psoriasis is thought to be related to an immune system issue with T-cells and other white blood cells, called neutrophils, in the body. T-cells normally travel through the body to defend against internal intruders, such as viruses or bacteria. But if you have psoriasis, the T-cells attack healthy skin cells by mistake, as if to heal a wound or to fight an infection, thus causing a scaly build-up of skin cells on the surface.
While it is considered a chronic condition, fortunately psoriasis can be managed through a variety of methods. Check out our top tips for managing psoriasis and its symptoms below!
-
Avoid Stressors
While stress is never 100% avoidable, you can give your body a fighting chance and help prevent psoriasis flare-ups by staying away from certain internal and external stressors. It’s a well-known fact that tobacco and alcohol can compromise even the healthiest of immune systems, but if you suffer from psoriasis, you’ll want to avoid that second glass of wine or after supper cigarette. Additionally, why you may not be able to avoid stress at work or home, adopting some easy stress release practices, such as yoga or meditation, may help reduce stress enough to prevent your immune system from going into overdrive.
-
Treat Your Skin Right
Did you know bathing or showering in hot water could make your psoriasis worse? Hot water is notorious for drying out the skin and causing flare-ups. We recommend soaking or showering in lukewarm water to help prevent a painful trigger. Additionally, a lukewarm bath with epsom salts, milk, or olive oil could help relieve the painful symptoms of psoriasis. In fact, mixing a tablespoon of olive oil with your body moisturizer actually helps to seal in essential moisture, and adds an additional layer of topical protection when applied to active psoriasis breakouts.
-
Consider Participating in a Clinical Trial
Modern medicine continues to make incredible strides in helping to manage psoriasis, with Jacksonville Center for Clinical Research on the front lines of exploring new and exciting treatments. Contact us to schedule a free consultation to see if you qualify for one of our clinical research studies. If you qualify for one of our clinical trials, your health will be closely monitored by our team of expert medical professionals throughout the trial. It is an accepted statistic that people who participate in clinical trials generally improve their overall health, as they are given access to cutting edge clinical techniques and healthcare experts dedicated to their individual needs.

Medical progress has made the lives of folks with autoimmune conditions such as psoriasis and psoriatic arthritis (PsA) better than ever before. These conditions have been extremely difficult to treat successfully in the past. Now thanks to advancements in medicine using biological agents more people are living free of psoriasis and PsA flare ups.
Psoriasis is most commonly known for the raised, white or greyish patches that appear on the skin. These patches can progress to thick, scale-like plaques which may harden and become cracked. The severity of psoriasis is measured both by how much psoriasis a person has on their body and how much it affects their quality of life. For example, psoriasis can have a serious impact on one’s daily activities even if it involves a small area, such as the palms of the hands or soles of the feet.
Psoriatic arthritis is an inflammatory form of arthritis affecting the joints and is often accompanied by skin psoriasis. Early diagnosis and treatment of PsA can help prevent or limit extensive joint damage that occurs in later stages of the disease. Symptoms are similar to the discomfort associated with osteoarthritis (OA). One way to tell the two conditions apart is determining whether the arthritis is symmetrical or not. PsA usually affects major joints of the body symmetrically, while OA commonly affects one particular joint such as the left knee or right hip. An accurate diagnosis may require x-rays and blood tests. Once diagnosed an effective treatment plan may begin.
In the past, doctors could only treat psoriasis topically and with limited success. In the 1950’s researchers discovered methotrexate, an immune suppressant, and in the 1970’s it was approved for use in patients not responding to topical treatments. This medication and others like it are still used today, however there can be many possible side effects when suppressing the immune system. Through many years of research and clinical trials, researchers have now discovered biologics. Biologics are genetically-engineered human or animal based proteins designed to target the specific inflammatory pathways caused by psoriasis and PsA. Because of the large molecule size and complexity of biologics, they must be injected in order to be absorbed. Fortunately, injections are only needed once a month or every several months to be effective in most cases. There are several biologics currently FDA approved, however because of the recent discovery and high production costs, biologics can be extremely expensive through insurance.
At Encore Research Group, we are currently investigating many new and exciting biologic drugs for psoriasis and psoriatic arthritis. We are actively looking for qualified participants in North East Florida. Research provides participants with many great benefits. Some advantages of participating in a study include cutting-edge therapies, study-related medication at no cost and a stipend for time and travel. If you are interested in learning more about research, or our current studies please visit our website for more information. Without participants today, there won’t be new medications tomorrow!