GRID VIEW
When we think of an animal, we generally think of a single creature with a unique DNA code. A human starts as a single fertilized egg cell with the combined genetic code from our parents. By the time we’re walking and talking, however, we’ve already transformed into a superorganism. If you were to count the number of cells that make you up, only half would be human. Mature red blood cells lack a nucleus, so if we count only cells with nuclei, we’re only about 10% human. Going further, if we count all the genetic material in our body, only about 1% of it is human. Genetically, we’re 99% nonhuman. So then, what are we? Bacteria. We’re primarily bacteria. These bacteria live with us our whole lives. They live on our skin, in our hair, on our eyelashes, and in our gut. The bacteria that live in the digestive tract, along with the relatively minuscule amounts of viruses, archaea, and yeasts, make up the gut microbiome. The gut microbiome is incredible. It establishes itself until around age two. It changes in response to the food we eat, diseases we get, medications we take (especially antibiotics), and our hygiene. We eat around 60 tons of food in our lives, and the gut microbiome has a hand in all of it. We usually think of bacteria (and viruses, etc) as parasitic (doing damage). The reality is the gut microbiome is truly symbiotic, we need it as much as it needs us. The gut microbiome performs many tasks for us. It shapes the human cells and the mucus that lines our gut, strengthening it. It protects us from infections, keeps our cells together in a tight barrier, and communicates with the immune system. Microbiome cells outcompete other, destructive bacteria. They can also release bacteriocins (bacteria-targeting toxins) that destroy dangerous bacteria. The microbiome is so stellar it helps us even when it’s just eating. The gut microbiome breaks down foods we can’t process, like dietary fiber. Through the process of fermentation, it uses this food to make vitamins, minerals, etc. As an example: we can’t make vitamin B12 at all in our cells; we rely on microorganisms to make it for us! Finally, the gut microbiome makes short-chain fatty acids. Short-chain fatty acids are the primary energy source for the human cells that line the intestine. They also increase insulin sensitivity and mediate immune regulation, inflammation, and other body processes. Unfortunately, the gut microbiome can get out of whack, and issues like ulcerative colitis – an inflammatory bowel disease – can occur. To understand what can go wrong, let’s first investigate a healthy gut microbiome. The colony of colon bacteria is unique in everyone. A healthy microbiome has three qualities: high diversity, high richness, and high stability. Diversity is just what it sounds like: the total number of different species present. Richness is the balance between species; having roughly equivalent numbers of bacteria from each. Stability is the consistency of finding the same types and numbers of organisms over time. So what does a disruption in the balance of the gut microbiome look like? Loss of diversity, overgrowth of some types of organisms, and changes to the composition of the gut microbiome over time. The degradation of diversity, richness, or stability is called dysbiosis. One cause of dysbiosis is antibiotics. They are designed to kill bacteria, which is bad news for the gut bacteria. Antibiotics frequently lead to a redistribution of gut microbiota. Other things that can cause dysbiosis include hygiene, infection, and smoking. The most important, however, is diet. All of the food we eat travels through the gut. In the western world, our diets aren’t always built to cultivate a healthy gut microbiome. Much of our food is built for shelf stability and is made using enzymes or chemicals instead of bacteria. We tend to eat more animal fats and proteins and fewer plant fibers than indigenous populations. To top this off, we eat refined sugar. Like, a LOT of refined sugar. Around 50 to 100 pounds of refined sugar per year. I’m not a nutrition expert, but I am a cookie expert, and that’s way too many cookies. When the microbiome is in a state of dysbiosis, it can’t perform its helpful functions. The mucus layer is reduced, bacteria can’t interact with the immune and inflammation systems, and the gut is more permeable to undesirable substances. On top of this, short-chain fatty acid production decreases, making it more difficult for the human cells lining the gut. This loss of function is linked to diseases like ulcerative colitis. The exact causes of ulcerative colitis are unknown, but scientists think it is related to the gut microbiome. Ulcerative colitis is a chronic inflammatory disease with periods of high and low activity. Inflammation leads to painful ulcers along the colon and rectum. So what can we do when the gut is out of whack? This is still a relatively new area of research, so there are many questions we have to answer. Our best solutions so far are food and feces. The importance of food to the gut microbiome should be obvious by now. Foods high in dietary fibers from plants are needed for gut bacteria to survive and thrive. The role of bacteria derived from human feces is still being developed. Fecal transplantation is a fascinating, but not-for-the-dinner-table line of study. The basic idea is that doctors would transfer some of the gut microbiome from a healthy person to a sick one, perhaps someone with ulcerative colitis. These bacteria would hopefully colonize and outcompete whatever is disrupting the sick microbiome, restoring diversity, richness, and stability. Focusing on the symbiotic relationship we share with our individual microbiome will revolutionize our approach to healthcare. Clinical trials may pave the way forward for treatments that support our human cells and our microbiome, nurturing the microbial communities vital to our survival and well-being as a superorganism. Also, don’t forget to eat your veggies. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Bengmark, S. (1998). Ecological control of the gastrointestinal tract. The role of probiotic flora. Gut, 42(1), 2-7. https://doi.org/10.1136/gut.42.1.2 Fan, Y., & Pedersen, O. (2021). Gut microbiota in human metabolic health and disease. Nature Reviews Microbiology, 19(1), 55-71. https://doi.org/10.1038/s41579-020-0433-9 Gomaa, E. Z. (2020). Human gut microbiota/microbiome in health and diseases: a review. Antonie Van Leeuwenhoek, 113(12), 2019-2040. https://link.springer.com/article/10.1007/s10482-020-01474-7 LeBlanc, J. F., Segal, J. P., de Campos Braz, L. M., & Hart, A. L. (2021). The microbiome as a therapy in pouchitis and ulcerative colitis. Nutrients, 13(6), 1780. https://doi.org/10.3390/nu13061780 Sender, R., Fuchs, S., & Milo, R. (2016). Revised estimates for the number of human and bacteria cells in the body. PLoS biology, 14(8), e1002533. https://doi.org/10.1371/journal.pbio.1002533 Świrkosz, G., Szczygieł, A., Logoń, K., Wrześniewska, M., & Gomułka, K. (2023). The Role of the Microbiome in the Pathogenesis and Treatment of Ulcerative Colitis—A Literature Review. Biomedicines, 11(12), 3144. https://doi.org/10.3390/biomedicines11123144 Tan, J., McKenzie, C., Potamitis, M., Thorburn, A. N., Mackay, C. R., & Macia, L. (2014). The role of short-chain fatty acids in health and disease. Advances in immunology, 121, 91-119. https://doi.org/10.1016/b978-0-12-800100-4.00003-9 The Human Microbiome Project Consortium. (2021). Structure, function and diversity of the healthy human microbiome. Nature 486, 207–214. https://www.nature.com/articles/nature11234 Thursby, E., & Juge, N. (2017). Introduction to the human gut microbiota. Biochemical journal, 474(11), 1823-1836. https://portlandpress.com/biochemj/article/474/11/1823/49429 Xiong, R. G., Zhou, D. D., Wu, S. X., Huang, S. Y., Saimaiti, A., Yang, Z. J., … & Li, H. B. (2022). Health benefits and side effects of short-chain fatty acids. Foods, 11(18), 2863. https://doi.org/10.3390%2Ffoods11182863 Young, V. B., & Schmidt, T. M. (2008). Overview of the gastrointestinal microbiota. Advances in experimental medicine and biology, 635, 29–40. https://doi.org/10.1007/978-0-387-09550-9_3
Listen to the article here:

High blood pressure is amazingly prevalent, affecting nearly half of all Americans. It’s a major risk factor for heart attack, stroke, kidney failure, eye damage, and more. Unfortunately, this condition remains highly prevalent despite the numerous medications designed to treat it. For many patients, adhering to medications can be difficult, and for others, some medicines are not effective in reducing blood pressure levels. But what if there were a way to lower blood pressure at the source, the heart? First, let’s examine how the heart relates to blood pressure. It might seem obvious, but it’s actually quite complex. The heart draws blood in and pushes it out with each beat. The amount of blood pumped is called the stroke volume. A good stroke volume helps to ensure the heart has enough blood pressure to deliver oxygen throughout the body. A healthy heart will pump out around 50-70% of the total volume of blood. This means there remains some unpumped fluid in the heart chambers after pumping is complete. When the next heartbeat comes, the heart muscle has to stretch enough to accommodate this unpumped blood. This extra blood increases our blood pressure because of the Frank-Starling law of the heart. The Frank-Starling law of the heart is over 100 years old and states that the amount our heart muscles stretch before pumping scales with the force they deliver when pumping. Think of a rubber band. If you stretch it a little, it’ll flop back in place. If you stretch a rubber band a lot, almost to its breaking point, it’ll snap back so hard as to leave a welt on your skin. The heart is similar; extra blood in the heart before pumping increases the pressure of each beat and maintains our blood pressure. If there were a way to lower the amount of blood in the chamber after beating, it follows that blood pressure may be lowered. Note that just the pressure would be lowered. The stroke volume would (ideally) remain the same. But how could we do this? For most people, we don’t have any way of convincing the heart to empty more effectively. For a select few, however, the hardware may already be in place. Pacemakers are amazing technology that has helped countless people whose hearts aren’t working properly. Over a million pacemakers are implanted every year worldwide and help people with arrhythmias. Arrhythmias are conditions that involve irregular heartbeat. Pacemakers are surgically implanted devices that send small amounts of electricity where they are needed in the heart. Heart muscles are triggered by this little zap and beat in response to it. Pacemaker rhythms can be customized for several types of conditions, and can even be programmed after being implanted to adapt to changing patient conditions. This is where a pacemaker’s ability to help with high blood pressure is theorized. By customizing how a pacemaker fires, it is possible to cause the heart to release more of its contents and lower the amount of blood remaining in the heart before pumping. According to the Frank-Starling law of the heart, this should result in lower blood pressure (indeed, early clinical trials show this to be the case). Finally, we have to make sure changes to our blood pressure bypass the sympathetic nervous system. This pathway, also called the “fight or flight” pathway, helps ensure the body is awake, alert, and alive. Integral to this system are receptors that sense our blood pressure. If the sympathetic nervous system senses a prolonged drop in blood pressure, it kicks in to correct this. This is a critical system that keeps us from constantly fainting but can be problematic when trying to lower blood pressure. A clever workaround being investigated is to have a pacemaker lower the blood pressure intermittently. It runs the chamber-emptying algorithm for short periods of time. This may help bypass our sympathetic nervous responses. If clinical trials bear out, pacemakers may be able to change not just the pace of the heart, but the pressure too! Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Centers for Disease Control and Prevention. (2023). Facts about hypertension. U.S. Department of Health & Human Services. https://www.cdc.gov/bloodpressure/facts.htm Mond, H. G., & Proclemer, A. (2011). The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: calendar year 2009–a World Society of Arrhythmia’s project. Pacing and clinical electrophysiology : PACE, 34(8), 1013–1027. https://doi.org/10.1111/j.1540-8159.2011.03150.x Kalarus, Z., Merkely, B., Neužil, P., Grabowski, M., Mitkowski, P., Marinskis, G., … & Kuck, K. H. (2021). Pacemaker‐Based Cardiac Neuromodulation Therapy in Patients With Hypertension: A Pilot Study. Journal of the American Heart Association, 10(16), e020492. https://www.ahajournals.org/doi/full/10.1161/JAHA.120.020492 Mitchell, L.B. (2023). Cardiac pacemakers. Merck Manual, Professional Version. https://www.merckmanuals.com/professional/cardiovascular-disorders/overview-of-arrhythmias-and-conduction-disorders/cardiac-pacemakers Neuzil, P., Merkely, B., Erglis, A., Marinskis, G., de Groot, J. R., Schmidinger, H., … & Kuck, K. H. (2017). Pacemaker‐mediated programmable hypertension control therapy. Journal of the American Heart Association, 6(12), e006974. https://www.ahajournals.org/doi/full/10.1161/JAHA.117.006974 Sequeira, V., & van der Velden, J. (2015). Historical perspective on heart function: the Frank–Starling Law. Biophysical reviews, 7, 421-447. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5418489
Listen to the article here:

One of the most important tasks for researchers is to make sure the experiment we are running is accurately assessing the intended variable. Because of this, each study has specific inclusion and exclusion criteria, which determine who can qualify to participate. An example would be needing a diagnosis of severe asthma for a study testing a new asthma medication. Usually, criteria include age, relevant medical diagnoses or histories, and exclude major health events such as cancer, heart attack, or stroke. Recently (as of the writing of this article), however, we have seen a notable uptick in the number of cardiovascular studies that allow or even require a previous heart attack or stroke as an inclusion criterion. This is because there are several medications or devices being studied that hope to lower the recurrence of these events. Heart attack and stroke are often two sides of the same coin. In both cases, blood flow to part of the organ is lowered or stopped, and the affected tissue is damaged or dies. You might be familiar with the term Major Adverse Cardiovascular Event (MACE), which encompasses various cardiovascular issues, including heart attack and stroke. Most people survive their first incident, but 20-25% of people have more than one. According to the American Heart Association, about 1 in 5 people who have had a heart attack will suffer from (or experience) a second one within five years. Each heart attack or stroke comes with a chance of lowered quality of life, disability, or death, so preventing further events is critical. One of the biggest problems with preventing a second heart attack or stroke is the myriad of causes of these conditions. Any prolonged insult to the cardiovascular system can lead to a heart attack or stroke. The risks, then, include a sedentary lifestyle, poor diet, obesity or excess weight (especially around the midsection), high blood pressure, high cholesterol, uncontrolled diabetes, smoking, stress, alcohol, and drugs. The solutions to these disparate causes can also spread far and wide. For this reason, the two most important ways to reduce the risk of a second heart attack or stroke are to talk to a medical professional and take prescribed medications. A medical professional can look at the underlying condition of individuals and determine which factors likely had the biggest impact. They may recommend cardiac rehabilitation and specific medications to address underlying conditions and prevent recurrence. Targeting specific, relevant causes with medications, such as anticoagulants like warfarin, antiplatelets like aspirin, and cholesterol-lowering medications like statins, can reduce the risk of resurgence by up to 70%! Doctors may also recommend medications to help with diabetes or blood pressure and/or surgical procedures to fix structural problems with the cardiovascular system. Managing the risk factors that caused the first heart attack or stroke can reduce the likelihood of a second (or third). On top of this, changes to lifestyle and diet can have a significant impact, lowering the chance of a second event by almost a third. Add a reduction in smoking, alcohol, and drugs for an even greater effect. Beyond standard medical advice, two additional interventions may help. The first is support. Family, friends, and others who have experienced heart attacks and strokes can help make the recovery process more bearable and lower anxiety and stress (which are risk factors in themselves!). Finally, clinical trials may help. Indeed, the inclusion of previous heart attacks or strokes in clinical research inclusion criteria indicates an increased recognition that indirect influence can induce repeated injury to the heart and brain. In short, research studies are looking at new ways to lower the incidence of a second heart attack or stroke by targeting underlying conditions with new medications and new methods of treatment. This is invariably a great idea. Only YOU (and your doctor (and maybe a clinical research coordinator)) can prevent secondary strokes and heart attacks. At the time of this writing, ENCORE Research Sites have several studies for people who have had a previous heart attack or stroke. Call your local office to explore research options for you. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Yoo, S. G. K., Chung, G. S., Bahendeka, S. K., Sibai, A. M., Damasceno, A., Farzadfar, F., … & Flood, D. (2023). Aspirin for Secondary Prevention of Cardiovascular Disease in 51 Low-, Middle-, and High-Income Countries. JAMA, 330(8), 715-724. https://doi.org/10.1001/jama.2023.12905 Esenwa, C., & Gutierrez, J. (2015). Secondary stroke prevention: challenges and solutions. Vascular health and risk management, 437-450. http://dx.doi.org/10.2147/VHRM.S63791 American Heart Association News. (April 4, 2019). Proactive steps can reduce chances of second heart attack. American Heart Association. https://www.heart.org/en/news/2019/04/04/proactive-steps-can-reduce-chances-of-second-heart-attack American Heart Association. (2022). 5 ways to lower your risk of a second heart attack. American Heart Association. https://www.heart.org/-/media/files/health-topics/heart-attack/5-ways-to-lower-your-risk-of-second-heart-attack-infographic.pdf Karlin, R., Wojcik, S., Kang, S. (2024). Preventing a second heart attack. University of Rochester Medical Center Rochester. https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=56&contentid=2446 de Jong, M., van der Worp, H. B., van der Graaf, Y., Visseren, F. L., & Westerink, J. (2017). Pioglitazone and the secondary prevention of cardiovascular disease. A meta-analysis of randomized-controlled trials. Cardiovascular diabetology, 16(1), 1-11 .https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5644073/
Scroll down to listen to this article.
Listen to the article here:

Heart failure is when the heart doesn’t pump enough blood throughout the body. This doesn’t mean instant death, but the body starts wearing out around the edges. People with heart failure might feel short of breath and tired because there’s not enough oxygen reaching the brain and cells. Ankles and lower extremities might start swelling because the heart is unable to pull all of the blood up out of our legs. Sufferers understandably have trouble exercising. So what’s going on? Can anything be done about it? Heart failure is an enormous problem. Tens of millions of people worldwide suffer from it, including at least 6 million Americans. It is the most common cause of hospitalization for adults over 65, and causes many repeat hospitalizations. Heart Failure severely reduces the quality of life, and comes with a high mortality rate. The causes of heart failure are numerous and can be difficult to identify; anything that impairs the heart’s ability to pump or deliver oxygen can be a contributing factor. Risk factors include: To understand how these conditions may contribute to heart failure, we should first dive wholeheartedly into how the heart works. The heart is a muscle. It squeezes about once a second in a coordinated fashion. This squeezing pushes blood to and from the lungs, and to and from the body. We generally don’t get new heart muscle cells as adults. Instead, in order to react to changes in the needs of the body the heart cells themselves can grow (enlarge), as can the structure around and between the cells. A healthy heart may get stronger and more efficient in response to exercise or pregnancy A weakened heart, on the other hand, might change its structure by enlarging in response to stress, hormone changes, inflammation, and/or the risk factors listed above. These changes can result in a reduction of the amount of capillaries that supply the heart with blood, as well as fibrosis, chemical changes, and changes in the metabolism and organization of heart cells. But why would the heart do this? Is it rebelling against us? Is it something I said? The heart loves us with its whole… self. It changes because it is trying its hardest and can’t manage to do it alone. When the heart senses it isn’t functioning properly, it may undergo cardiac hypertrophy. Cardiac is Greek (and Latin (and French)) for heart. Hyper- indicates an excessive amount, and -trophy is from the Greek word for nourishment, which in this case means growth. Cardiac hypertrophy is the excessive thickening or lengthening (or both) of the heart muscle. In pathological heart disease, scientists think this is initially an adaptive response. The heart attempts to compensate for dysfunction by increasing the size of the heart tissue. This works for a bit, right up until it doesn’t. Eventually, blood vessels can no longer reach all of the heart tissue. As a result, important chemicals like nitrous oxide are not produced and delivered to cells, connective tissue grows and stiffens, hormones get out of balance, and damaging inflammation occurs. These maladaptive signs of heart failure give evidence as to why it’s so dangerous. Each of these responses to a stressed heart can also cause damage and restructuring of the heart. Inflammation is a great example. Consistent inflammatory chemicals in the body can spur the heart into a stress response that results in structural changes, which in turn may cause inflammation that spreads to other parts of the body. Similarly we can look at hormones like angiotensin, which regulate blood pressure by affecting how narrow your blood vessels are. An excess of angiotensin can narrow blood vessels and cause the heart to work harder, leading to thickening of the tissue. However, when the stiff tissue doesn’t pump blood efficiently the body responds by releasing more angiotensin in an attempt to help blood move through the body. Regardless of the initial cause, when the heart can’t keep up with the demands of the body, heart failure occurs. So what can be done? Luckily, this problem has attracted some of the best minds on the planet (like our very own Dr. Michael Koren). Standard treatments aim to improve the quality of life and heart function in patients while reducing the incidence of hospitalization and mortality. Four classes of medications make up the standard of care (SOC) for heart failure: These SOC medications, though effective in many patients, are not perfect. While they tend to target and counteract the effects of wayward hormones, they do not address underlying heart dysfunction or the changes to heart structure occurring beneath it all. There are many new medications that target a host of new mechanisms for fighting the scourge of heart failure. These include targeting the inflammation pathways or simulating the effects of relaxin. Relaxin is a natural hormone with many effects, including recycling extra structural material in the heart and increasing the efficiency of heart muscle at the tissue level. With luck (and the help of excellent, well-read volunteers like yourself), we can turn heart failure into heart success. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Groenewegen, A., Rutten, F. H., Mosterd, A., & Hoes, A. W. (2020). Epidemiology of heart failure. European journal of heart failure, 22(8), 1342-1356. https://doi.org/10.1002/ejhf.1858 Lopaschuk, G. D., & Verma, S. (2020). Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: a state-of-the-art review. Basic to Translational Science, 5(6), 632-644. https://doi.org/10.1016%2Fj.jacbts.2020.02.004 Murphy, S. P., Kakkar, R., McCarthy, C. P., & Januzzi Jr, J. L. (2020). Inflammation in heart failure: JACC state-of-the-art review. Journal of the American College of Cardiology, 75(11), 1324-1340. https://doi.org/10.1016/j.jacc.2020.01.014 Pandey, K. N. (2008). Emerging roles of natriuretic peptides and their receptors in pathophysiology of hypertension and cardiovascular regulation. Journal of the American Society of Hypertension, 2(4), 210-226. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2739409/ Shimizu, I., & Minamino, T. (2016). Physiological and pathological cardiac hypertrophy. Journal of molecular and cellular cardiology, 97, 245-262. https://doi.org/10.1016/j.yjmcc.2016.06.001 Xie, Y., Wei, Y., Li, D., Pu, J., Ding, H., & Zhang, X. (2022). Mechanisms of SGLT2 inhibitors in heart failure and their clinical value. Journal of Cardiovascular Pharmacology, 10-1097. https://doi.org/10.1097/FJC.0000000000001380
Scroll down to listen to this article.
Listen to the article here:
Electricity is essential for most modern-day activities. We use it for lights, air conditioning, and watching cat videos. We also use it to keep our hearts beating. Electricity coordinates the heart and causes it to contract into its familiar wub-dub. Why do we need electricity in the heart, and what can we do when the zips don’t zap properly? Shockingly, we’ll start with a broad overview. The heart is an organ made of several billion cells. These are organized into many structures, including chambers. There are two small upper chambers called atria, which is the plural word for the left atrium and right atrium. There are also two large lower chambers called ventricles, which are again separated into left and right. The set on the left pumps fresh, oxygenated blood from the lungs to all the cells in the body. The set on the right pumps deoxygenated blood to the lungs to get more oxygen. It is a little strange to describe the heart only as a series of chambers, as the actual structure of the heart is a giant, very strong, coiled muscle. In order for muscles to contract and produce power, electricity is needed. Electricity tells the muscles they need to move. In most of the body, the electrical signals for muscles to contract are delivered by the brain. The heart is a little different. The heart is involuntary, meaning we have no direct control over when it beats. We can send signals to the heart by breathing deeply or jumping, but the electrical signal that tells the heart to beat comes from within the heart itself. Near the top is a collection of cells called the sinoatrial (SA) node. Here resides a group of cells called pacemaker cells. These cells produce a small electrical zippy zappy signal around once per second. This signal rapidly amplifies and spreads throughout the atria, causing them to contract. This spreading comes out like a wave, which allows all the atrial muscle cells to contract in a big, coordinated manner. Soon after, the signal travels through the atrioventricular (AV) node into the ventricles, propagating outward. This takes a fraction of a second, so we hear wub-dub instead of just one big beat. This also gives blood time to travel from the atria to the ventricles, ensuring it goes correctly. This system is pretty amazing, but it’s not foolproof. Many things can go wrong. The electrical signal might be disrupted, the heart might be too slow, or it might beat at a bizarre rhythm. When this happens, the heart pumps less efficiently than it needs to, and sometimes can’t pump enough blood for oxygen to get around the body. Unlike a heart attack, where heart cells die immediately, electrical problems can often be alleviated. When the electricity in our heart doesn’t behave correctly, we can put in artificial electricity. When the heart’s pacemaker cells aren’t successfully sending coordinated signals to the whole heart, an artificial cardiac pacemaker (often just called a pacemaker) can be implanted. Temporary pacemakers may sit outside the body, but permanent ones are installed inside our body cavities. These are made of materials our bodies don’t find threatening, like titanium. They can be attached to the heart through wires called leads, mounted on the heart surface, or inside the heart muscle. Each patient will have electrical problems in specific areas; maybe the pacemaker cells aren’t working properly, or maybe electricity can’t travel to the ventricles, or maybe it can’t cross from the left to the right side. Because of this, pacemakers can attach to either an atrium, a ventricle, or to both ventricles. Because the electrical problems are so varied, artificial pacemakers have many different patterns for firing. Artificial pacemakers don’t just cause beating; they also detect it. Little electrodes can tell when the heart has fired, and internal circuitry can measure this against when the cardiologist thinks a beat should have happened. Most will detect when a shock is needed and fire on demand, but some fire all the time. Pacemakers can respond to changes in heart rate, can sense abnormal rhythms, and have special modes for things like surgery. On top of all of this, medical professionals can often remotely monitor artificial pacemakers and adjust the pacemaker’s programming without surgery! This can be used to make sure heart rhythms stay ideal, but can also help alleviate the side effects of artificial pacemakers, which include chest pain, dizziness, fatigue, and shortness of breath. Pacemakers are amazing wonders of the modern era. As time goes on, scientists are developing new and more specific programs to zap the heart without zapping our fun. It’s nice to know that when you watch a video of a funny cat falling off the dresser, electricity makes your heart happy inside and out. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Buckberg, G. D., Nanda, N. C., Nguyen, C., & Kocica, M. J. (2018). What is the heart? Anatomy, function, pathophysiology, and misconceptions. Journal of cardiovascular development and disease, 5(2), 33. https://www.mdpi.com/2308-3425/5/2/33 Lak, H. M., & Goyal, A. (2020). Pacemaker types and selection. https://www.ncbi.nlm.nih.gov/books/NBK556011/ Sundnes, J., Lines, G. T., Cai, X., Nielsen, B. F., Mardal, K. A., & Tveito, A. (2007). Computing the electrical activity in the heart (Vol. 1). Springer Science & Business Media.
Scroll down to listen to this article.
Listen to the article here:

I recently went to a dessert party. That’s a party where everyone brings a dessert. I, naturally, arrived with cookies while others brought cakes and pies. Surprisingly, there was one attendee who presented a bowl of berries, another who showcased a sweet potato casserole, and a third who simply brought avocado with a dash of salt. Do these all count as desserts? What is a dessert? A word that was clear at the outset was quickly confusing in how broad it was. Unfortunately, that confusion can also happen with medical terms. Take cardiovascular disease. It’s got something to do with the heart, but sometimes it includes strokes in the brain. So what is cardiovascular disease? “Cardiovascular” is a word made of two component parts: cardio- means “heart” and vascular indicates blood vessels. Together, cardiovascular disease is that which affects the heart and/or blood vessels. The heart and blood vessels carry oxygen to the cells and keep them alive. Since we’re made of cells, keeping them alive is pretty important. Therefore, the heart and blood vessels are also quite important, and cardiovascular disease can be dangerous if not managed. Cardiovascular disease is more common than apple pie in the United States. Data from the CDC show that nearly HALF of adults over 20 have some form of cardiovascular disease. With a prevalence that high, it’s no surprise that cardiovascular disease is the leading cause of death in America and around the world. Unfortunately, as noted above, the exact definition of “cardiovascular disease” is very broad. In researching this article you are currently reading, I consulted the World Health Organization, the American Heart Association, and the National Institute of Health (part of the CDC). These organizations listed the various diseases included in cardiovascular disease, and only agreed on two conditions: Other diseases that at least two agreed on include: Though all these diseases may seem different, they are all part of the same system. Narrow blood vessels to the heart or brain cause oxygen loss. This narrowing can be caused by plaque formed when cholesterol lodges in the vessel wall. If some of this plaque dislodges, it can lead to heart attacks and strokes. Irregular heartbeats and heart attacks can lower the amount of blood (and oxygen!) delivered around the body. Hypertension stresses the whole system and can lead to heart attack, stroke, and damage to other organs like the kidneys. Additionally, they may have similar risk factors, outcomes, and treatments. There is a genetic component to cardiovascular disease. This is evident with congenital heart defects, which occur during development. It is also evident looking at who is at risk of developing cardiovascular disease. African Americans are at the highest risk, while people who identify as Hispanic have the lowest risk. Big modifiable risks include cholesterol, smoking, and hypertension (which is itself a form of cardiovascular disease!). Other risks include diabetes, being overweight, poor diet, low exercise, alcohol consumption, and low sleep. Research is ongoing into the cycle of mental health and cardiovascular disease as well. Mood and anxiety disorders, PTSD, and chronic stress can cause direct damage to the cardiovascular system while simultaneously increasing behaviors that compound the danger, including smoking and failing to take medicines. Lowering the modifiable risks above is, unsurprisingly, one of the best ways to fight cardiovascular disease. Managing cholesterol, blood pressure, and diabetes can help. Cutting smoking and lowering alcohol intake can make a big difference. Getting help with mental health (and getting a good night’s sleep) may help your heart relax as well. Maintaining a healthy weight through a good diet and dynamic exercise is vital. Unfortunately, without management, cardiovascular disease is more like a desert than a dessert: it can kill you. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Centers for Disease Control and Prevention. (July 19, 2021). Coronary artery disease (CAD). U.S. Department of Health and Human Services. https://www.cdc.gov/heartdisease/coronary_ad.htm National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention. (May 15, 2023). About heart disease. U.S. Department of Health and Human Services. https://www.cdc.gov/heartdisease/about.htm American Heart Association. (May 31, 2017). What is cardiovascular disease? https://www.heart.org/en/health-topics/consumer-healthcare/what-is-cardiovascular-disease Tsao, C. W., Aday, A. W., Almarzooq, Z. I., Alonso, A., Beaton, A. Z., Bittencourt, M. S., … & American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. (2022). Heart disease and stroke statistics—2022 update: a report from the American Heart Association. Circulation, 145(8), e153-e639. https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000001123 National Heart, Lung, and Blood Institute. (n.d). Heart and vascular diseases. U.S. Department of Health and Human Services. https://www.nhlbi.nih.gov/science/heart-and-vascular-diseases Accessed on September 12, 2023. The World Health Organization. (June 11, 2021). Cardiovascular diseases (CVD). https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
Scroll down to listen to this article.
Listen to the article here:
What do Star Wars, Nazi-occupied France, and surge protectors have in common? We root for the resistance to win! But what if the resistance is evil and bad? Meet resistant hypertension. This little devil is a special, particularly damning form of hypertension that resists medications. Not just one or two medications, either! Resistant hypertension avoids at least three separate medications of three separate types (called classes)! Resistant hypertension is when blood pressure remains over 140/90 mmHg while seated, even when the patient is taking the maximum tolerated dose of three or more different classes of hypertension medications. It can damage the heart, eyes, and kidneys and lead to heart attack, stroke, end-stage renal disease, and death. It can be caused by a narrowing of the veins, but the prevalence isn’t narrow at all. It affects 6-9 million Americans, with the highest incidence in Black males. A few conditions are associated with resistant hypertension, including diabetes, obesity, and chronic kidney disease. To understand how this disease works, we must first understand how blood pressure works. Blood pressure is controlled by three main components: heart rate, volume pumped, and blood vessel size. This may seem like a simple system, but each of these three components are affected by a myriad of body systems. Think of it like trying to maintain peace in the middle east. It might seem like you could balance the needs of religion, economics, tradition, and foreign influence, but it turns out: no. Other big actors in the blood pressure realm include the brain and kidneys. The brain directs other organs how to act and the kidneys regulate the fluid in the bloodstream (which we call blood). On top of these big organs, blood pressure is affected by interconnected systems, genes, inflammation, salt, even the bacteria in our gut! One of the biggest systems involved with blood pressure is the Renin-Angiotensin-Aldosterone System, or RAAS (or RAS). This system involves the kidneys and uses hormones to regulate blood pressure. It relies on a few key hormones and enzymes, and is also affected by other systems like the natriuretic peptide system and the brain. In hypertension, one or more of these systems no longer functions properly. We have four major classes of medication to help get the body back on track. Long-acting calcium channel blockers (CCB) reduce the amount that the heart and arteries can contract, relaxing the system. Angiotensin is a hormone that causes blood vessels to narrow. Angiotensin-converting enzyme inhibitors (ACEI) block angiotensin from being made and angiotensin receptor blockers (ARB) block it from acting on blood vessels. Finally, diuretic medications remove water and salt from the blood, lowering the volume of fluid that the heart pumps. Each of these medications targets the body in slightly different ways. Different medications work better for some people, and side effects may present differently. A good doctor will look for a blood pressure medication (or two (or three (or more))) that brings blood pressure to healthy levels without too many side effects. When we do not achieve healthy blood pressure levels even at the maximum tolerated dose of three or more medications we have resistant hypertension. Patients with resistant hypertension are at a higher risk of major cardiac events because they can’t get blood pressure under control with available medications. Prolonged high blood pressure leads to damage throughout the cardiovascular system. So what can be done? The best first step is to lower modifiable risks. This is actually a good first step for literally anything that is dangerous. Weight loss is a good opening move if you are obese. Lowering alcohol and salt intake may help. Talking to a doctor about any medications or conditions that may be raising blood pressure is important. Finally, clinical trials may be underway to look for specialty medications that target those with resistant hypertension. Hopefully we can find a way to crush resistance without succumbing to the dark side of the force (or becoming nazis). Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Harrison, D. G., Coffman, T. M., & Wilcox, C. S. (2021). Pathophysiology of hypertension: the mosaic theory and beyond. Circulation research, 128(7), 847-863. https://doi.org/10.1161/CIRCRESAHA.121.318082 Myat, A., Redwood, S. R., Qureshi, A. C., Spertus, J. A., & Williams, B. (2012). Resistant hypertension. Bmj, 345. https://doi.org/10.1136/bmj.e7473 Sarafidis, P. A., Georgianos, P., & Bakris, G. L. (2013). Resistant hypertension—its identification and epidemiology. Nature Reviews Nephrology, 9(1), 51-58. https://www.nature.com/articles/nrneph.2012.260
Listen to the article here:

Sometimes when I’m desperately trying to fall asleep I instead think of all the things that might kill me. Alligators, drunk drivers, hurricanes, and running out of cookies usually top the list. Do you know what doesn’t top the list? High blood pressure. It really should though. High blood pressure is a leading preventable cause of premature death, affecting well over a billion people worldwide and causing upwards of 9 million deaths a year. Maybe the alligators can chew on those facts for a while. So what is high blood pressure, why is it such a big deal, why do we get it, and what can we do? High blood pressure is exactly what it sounds like; when the blood in your arteries is being forced through more strongly than normal. The medical name for high blood pressure is hypertension. Hyper– means over or above, and -tension, in this case, indicates the stress of your arteries. Hypertension is excessive stress on your arteries. Blood pressure can be split into two numbers, systolic and diastolic. These refer to the action of the heart, where systolic is the contracted, pumping blood pressure, and diastolic is the relaxed blood pressure. When you get your blood pressure checked, these are reported as two numbers “over” each other. A reading of 140/90 mmHg or higher is high blood pressure, but there is an increased risk of complications with blood pressure above 120/80 mmHg. High blood pressure is particularly dangerous. It is easy to see why: the bloodstream is how we deliver oxygen to the cells, and it touches every cell in the entire body. Two of the biggest dangers with elevated blood pressure are ischemic heart disease and stroke, conditions where the blood supply doesn’t reach the heart or brain. High blood pressure can also cause brain bleeds, chronic kidney damage, and other types of heart damage. All of these organs are vital to our survival, so a condition that potentially damages all of them is life-threatening. What are the causes of high blood pressure? High blood pressure is calculated the same as in any pipe at its most basic level. The amount of blood coming out of the heart is counteracted by the resistance from the arteries. More output or more resistance makes blood pressure rise. High blood pressure on its own isn’t bad, it’s adaptive for critical situations. When we see a lion and it charges us, we become stressed and initiate the sympathetic nervous system, also known as fight, flight, and freeze. Part of this system’s job is to constrict blood vessels and raise the heart rate to deliver large amounts of oxygen to cells. We see damage when we have high blood pressure for long amounts of time. Some body systems that cause prolonged elevations in blood pressure are: These are the major players in primary or essential hypertension. Secondary hypertension is caused by another identifiable disease, like kidney disease. So what can we do? Some outcomes depend on things we can’t easily change, like access to quality healthcare and blood pressure medication. Many lifestyle options can be changed to improve our blood pressure: Even though we have good evidence for lifestyle changes lowering blood pressure, the biggest difference between countries in terms of controlling blood pressure is access to medicine. Blood pressure medicines have saved countless lives and helped stem the blood tide of hypertension. There are several types of blood pressure medicines on the market. Diuretics get rid of sodium and water in the blood. Angiotensin-converting-enzyme (ACE) inhibitors and Angiotensin-receptor blockers (ARB) help ease inflammation, relax the blood vessels, and keep them from constricting. Calcium channel blockers reduce heart rate. These all have side effects, but the biggest challenge with them is that they are daily oral medications, which can be forgotten, missed, or hard to adhere to. Longer-term solutions are in clinical trials and may be available to you if you qualify. So don’t sleep on your high blood pressure. Check with your local ENCORE Research office to see what studies are enrolling. See ya’ later, alligators! Staff Writer / Editor Benton Lowey-Ball, BS, BFA
Sources: Harrison, D. G., Coffman, T. M., & Wilcox, C. S. (2021). Pathophysiology of hypertension: the mosaic theory and beyond. Circulation research, 128(7), 847-863. https://www.ahajournals.org/doi/full/10.1161/CIRCRESAHA.121.318082 Lifton, R. P., Gharavi, A. G., & Geller, D. S. (2001). Molecular mechanisms of human hypertension. Cell, 104(4), 545-556. https://doi.org/10.1016/S0092-8674(01)00241-0 Mills, K. T., Stefanescu, A., & He, J. (2020). The global epidemiology of hypertension. Nature Reviews Nephrology, 16(4), 223-237. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7998524/
Listen to the article here:
Atrial fibrillation (AFib) is a heart rhythm disorder characterized by irregular heartbeats in the heart’s upper chambers, called the atria. In AFib, the electrical signals that regulate the heartbeat become abnormal, causing the heart to beat too fast or slow instead of contracting normally. Atrial fibrillation can have detrimental effects such as stroke, heart failure, and blood clots.
Image Credit: cdc.gov
As a result of the irregular heart beatings, a variety of symptoms can be present such as: In some cases, people with AFib may not experience any symptoms, making it difficult for some people to tell whether or not they may have AFib. Some broader symptoms can include: Sometimes even these broader symptoms can not help people determine if they have AFib. The only way for people to know if they have AFib without experiencing any symptoms is to get tested and diagnosed by a doctor. It is strongly recommended that if a person has any of the risk factors below, they get checked, just to be safe, by a doctor. AFib is often seen in older adults, with risk factors that include: Some treatments are more effective when delivered in the early stages of AFib, which means that a person should not postpone getting checked by a doctor for AFib. However, symptoms and causes of AFib can often differ between men and women. In women, AFib usually is caused by problems with the heart valves. Compared to men, where AFib usually stems from coronary artery disease (CAD). As a result, women with AFib have a greater chance of having a stroke than men with AFib. Women with AFib also are more likely to have heart attacks and congestive heart failure than men with AFib. As a result, treatments for men and women often differ slightly. Treatment for AFib is typically a medication to control heart rhythm and prevent blood clots. However, in some cases, procedures such as electrical cardioversion, ablation, or implantation of a pacemaker or defibrillator may be necessary. Men with AFib are often placed on non-drug therapies such as pacemakers and catheter ablation. Women with AFib are more likely to have a cardioversion and be prescribed antiarrhythmic medications such as dofetilide. However, typical treatments for both men and women include blood-thinning medications, surgery, and lifestyle changes to manage AFib risk factors. Written by: Sofia H. Davila, Clinical Researcher
Sources: Miller, K. (2022, December 27). Atrial fibrillation: The difference between men and women. Healthgrades. Retrieved February 17, 2023, from https://www.healthgrades.com/right-care/atrial-fibrillation/atrial-fibrillation-the-difference-between-men-and-women Centers for Disease Control and Prevention. (2022, October 14). Atrial fibrillation. Centers for Disease Control and Prevention. Retrieved February 17, 2023, from https://www.cdc.gov/heartdisease/atrial_fibrillation.htm


In the 1990’s the philosopher Haddaway posed a critical question: What is love? This Valentine’s Day, many of us will experience love and companionship. We like to think of love as an amorphous, idealistic quality, but there are serious biological underpinnings. What is the biology behind love, and is the heart really where love lies (spoiler: maybe?) We know that the brain directs our physical actions, but for the brain to come up with an idea, it needs input from the outside world. Interestingly, the brain can’t sense anything directly. If someone were to open up your skull and have a poke around, you would undoubtedly have a weird bit of sensation, but you wouldn’t experience the feeling of touch on the brain. We need special sensors (usually located on the skin) to feel things like touch. Indeed, our brain relies on signals coming in from all over the body to tell us about the outside world. Interestingly, we also rely on signals to tell us about the inside world – what we are experiencing. The brain interprets signals from the body, and we can experience that interpretation as an emotion. As an example: your heart beats automatically all day, every day, at a hopefully regular interval of around once a second. When you see a scary event, such as a wild lion charging you, your brain and body respond in sync. The heart rhythm changes, beating much faster to provide your muscles, sensory organs, brain, etc., extra oxygen in order to move fast. But this effect isn’t strictly rational. After we escape from the lion, we still feel “amped up.” This effect can last for thirty minutes or so, and the reason for the long-lasting effect is complicated. Our autonomic nervous system – the one in charge of things we don’t consciously control – has kicked into action. This pathway acts like cupid, shooting cortisol through our body and activating special nervous system pathways that take a while to cool down. But our brain also looks at the state of our body to interpret our emotional state. If our palms are sweaty, we’re breathing heavily, and our heart is racing, the brain interprets that as being amped up and decides we’re still pretty excited or scared. The brain is in charge of deciphering which emotion we’re feeling, but the body lets us know how strongly we’re feeling that emotion. This is why we sometimes still feel the need to continue an argument after the other party has conceded. It’s why telling someone to “calm down” doesn’t work – but taking some deep breaths does. Meditation, stretching, exercise, and sleep all affect our emotional state because the brain looks at the condition of the body and tries to figure out how it’s feeling. In addition, a healthy heart that can respond well to changes may increase a person’s emotional regulation. Does it do this with love as well? According to neuroendocrinology researcher Robert Sapolsky, it does! The science may not be entirely clear, but the easiest way to be certain of this is by looking at the irrationality of love. Love doesn’t make sense, and it’s so strong that we base enormous portions of our life just on this single emotion. Love is the basis of countless pieces of art, works of literature, grand buildings, and justifications for war. When we experience love – that fluttering of the heart, the excitement and elation, the involuntary smile on our face, and the giddiness so high that our mouths stop working and we say embarrassing, cheesy things – it’s the body to blame. Our heart races when we’re in love and the brain sees this as a huge exciting event – because it is. Just seeing the person we love can change our heart rate. Physical touch from a loving partner can help lower our heart rate in response to stressful situations. And the long-term effects of companionship sometimes include a partial synchronization of our heart rhythms. We can thank our hearts for at least some of what we call love. This Valentine’s day, get your heart racing with a partner or loved one, and keep that heart beating strong! By Benton Lowey-Ball, BS Behavioral Neuroscience
Ditzen, B., Neumann, I. D., Bodenmann, G., von Dawans, B., Turner, R. A., Ehlert, U., & Heinrichs, M. (2007). Effects of different kinds of couple interaction on cortisol and heart rate responses to stress in women. Psychoneuroendocrinology, 32(5), 565-574. https://doi.org/10.1016/j.psyneuen.2007.03.011 Kandel, E. R., Schwartz, J. H., Jessell, T. M., Siegelbaum, S., Hudspeth, A. J., & Mack, S. (Eds.). (2000). Principles of neural science (Vol. 4, p. 980). New York: McGraw-hill. Mather, M., & Thayer, J. F. (2018). How heart rate variability affects emotion regulation brain networks. Current opinion in behavioral sciences, 19, 98-104. Sapolsky, RM. (various works)
Listen to the article here:

Cardiovascular disease (CVD) is the leading cause of death in the United States. There are several risk factors for cardiovascular disease. This can include things you can’t change, such as sex, age, and genetics. They can also include things you can change. The WHO identifies four big behaviors that can change your risk of developing CVD: These behaviors generally lead to other undesirable indicators of health, including obesity, hypertension, high blood sugar, and increased cholesterol. Clearly, ceasing the behavioral risks is a high priority. Unfortunately, this is often easier said than done. One of the most difficult habits to quit is smoking. Studies show that those attempting to quit without assistance have an over 90% relapse rate. Several medications exist to help quit smoking, including Bupropion SR (aka Wellbutrin) and Varenicline (aka Chantix). There are also nicotine-based alternatives, including gum, inhalers, lozenges, nasal sprays, and patches. Nicotine rewires the brain as it’s consumed. It releases dopamine, the brain’s reward drug, and rewards us for smoking. Researchers think the frequency of smoking may be partially to blame for the intensity of the addiction. The amount of dopamine released is not particularly high compared with other drugs, but nicotine also causes changes to the striatum. The striatum is part of the reward circuit in the brain. Through a complicated mechanism, nicotine increases the amount of a protein called FosB, which changes the striatum’s sensitivity to dopamine. This is a change at the genetic level which makes the brain more susceptible to further reward signals. Nicotine seems to make normal activities more pleasurable. Unfortunately, as nicotine adjusts the brain’s mechanisms, the brain relies on it to get to a baseline of reward. Upon quitting smoking, the brain finds normal activities less enjoyable. On its own, nicotine may have negative effects, and in heavy doses it has been shown to be dangerous. The biggest dangers of smoking, however, are likely in the myriad of other chemicals in tobacco and cigarettes. Though nicotine causes changes in the brain, cigarettes cause changes to the fats in your body, further increasing CVD risk. Along with this, cigarettes cause cancer, COPD, diabetes, erectile dysfunction, and immune system changes. Clearly, quitting smoking is critical to health. With the addictive nature of nicotine and the low success rate of quitting cold turkey, assistance may be needed. The brain gets addicted to nicotine, but we can fight back using behavior. You can actually help yourself “break the cycle” of nicotine addiction by changing your daily routines. For example if the first thing you do in the morning is reach for a cigarette, change your routine to going to the bathroom and brushing your teeth first instead. Behavioral interventions can make a significant difference. Combining behavior changes and counseling with a nicotine replacement or medication can help quit rates approach 30%. Indeed, nicotine replacements are most effective when used with behavioral interventions. Changing your behavior or routine can have positive impacts on your health. So next time you want to reach for a cigarette, grab your phone instead! Give us a call and discover what clinical trials you can take part in!
Sources: Bancej, C., O’Loughlin, J., Platt, R. W., Paradis, G., & Gervais, A. (2007). Smoking cessation attempts among adolescent smokers: a systematic review of prevalence studies. Tobacco control, 16(6), e8-e8. https://doi.org/10.1136%2Ftc.2006.018853 Fiore, M. (2008). Treating tobacco use and dependence; 2008 guideline. https://stacks.cdc.gov/view/cdc/6964/cdc_6964_DS1.pdf Garbin, U., Fratta Pasini, A., Stranieri, C., Cominacini, M., Pasini, A., Manfro, S., … & Cominacini, L. (2009). Cigarette smoking blocks the protective expression of Nrf2/ARE pathway in peripheral mononuclear cells of young heavy smokers favouring inflammation. PloS one, 4(12), e8225. https://doi.org/10.1371/journal.pone.0008225 Koren, M. (Host). (2022, May 22). Nicotine replacement therapies to help stop smoking [Audio podcast episode]. In Medevidence! Truth behind the data. ENCORE Research Group. https://www.buzzsprout.com/1926091/10484183-nicotine-replacement-therapies-to-help-stop-smoking Messner, B., & Bernhard, D. (2014). Smoking and cardiovascular disease: mechanisms of endothelial dysfunction and early atherogenesis. Arteriosclerosis, thrombosis, and vascular biology, 34(3), 509-515. https://doi.org/10.1161/ATVBAHA.113.300156 NIDA. (2018, September 28). Recent Research Sheds New Light on Why Nicotine is So Addictive. https://nida.nih.gov/about-nida/noras-blog/2018/09/recent-research-sheds-new-light-why-nicotine-so-addictive US Department of Health and Human Services. (2014). The health consequences of smoking—50 years of progress: a report of the Surgeon General. https://www.ncbi.nlm.nih.gov/books/NBK294320/
Listen to the article here:

The familiar wub-dub of the heart accompanies us throughout our lives, providing a gentle beat that keeps us alive. But for some of us, the beat might not be so steady. For 33 million people worldwide, the heartbeat lacks a rhythm at all. It sounds like shoes in a clothes dryer and gets progressively worse. This is called Atrial Fibrillation, or AFib for short. The risks of AFib increase with age, and there is a genetic component as well. Other risk factors include: In order for AFib to occur, doctors believe there needs to be a trigger and a substrate. A trigger, or driver, is the electric signal that travels to the heart and initiates an arrhythmic event. This can be from several areas, but is frequently from one of the big pulmonary veins that carry oxygen to the heart. A substrate is the underlying condition that makes a sustained event possible and could be structural or electrical. Common substrates include the electrical system of the heart, dilation (or stretching) of the atrium, cellular-molecular changes, and/or an increase in disruptive cells called fibroblasts. In general, many or all of these changes would occur, leading to constant AFib. AFib is very dangerous. Other than a wonky pulse, there are three major complications: heart failure, stroke, and myocardial infarction (a heart attack). Heart failure is when the heart can’t pump enough blood, while stroke and myocardial infarction can be caused by stray blood clots. Heart failure is both a risk and a symptom, which illustrates one way in which AFib is a progressive disease. Through complicated electric and biocellular mechanisms, long term AFib seems to cause more AFib. Treating AFib has proven difficult. It is effective to treat the underlying risk factors, such as obesity and diabetes, but this is difficult and the actual cause of AFib isn’t always clear. Controlling the rhythm of the heart is also tough and risky, as messing with heart rhythm can easily lead to big problems. Atrial fibrillation ablation is an effective treatment. It is an intensive surgical procedure where doctors scar problem areas to reduce electrical activity. Even with this method, the risk of resurgence is over 30% after 5 years. Two of the biggest complications of AFib are related to blood clots. Because of this – and the difficulty of other treatments – major pharmaceuticals often target thromboembolisms, or clots. The clotting system itself is very complicated. A simple version is that platelets activate and produce several enzymes. These enzymes make thrombin, which makes a big mesh-like protein called fibrin. This would be a slow process, except that thrombin also activates amplifier enzymes, which makes this process very fast. The fibrin then catches red blood cells and blocks wounds – or blood vessels. When these clots travel to the brain they can cause a stroke. When they restrict blood flow to the heart they can cause a myocardial infarction – a heart attack. Classic anticoagulants, such as Warfarin (also called Jantoven and Coumadin) work by stopping the clots before they start. These are Vitamin K dependent anticoagulants and can be effective at reducing clots. Unfortunately, they are occasionally too effective. The biggest side effect of Vitamin K dependent anticoagulants is increased bleeding. This can be a serious problem for several patients, including high-risk older patients. Doctors are investigating new classes of medications which do not depend on vitamin K. These are called Non-vitamin K oral anticoagulants (NOACs) and some target the amplification pathway of clotting instead. There are currently four FDA-approved NOAC drugs on the market; dabigatran (Pradaxa), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa). Thrombin and fibrin still get produced and some clotting can occur, but the rapid amplification is shut down. The hope is that this can allow the body to repair trauma and stop external bleeds without building internal clots from AFib. With your help and participation in clinical trials, we can push science without pushing clots. By Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Iwasaki, Y. K., Nishida, K., Kato, T., & Nattel, S. (2011). Atrial fibrillation pathophysiology: implications for management. Circulation, 124(20), 2264-2274. https://doi.org/10.1161/CIRCULATIONAHA.111.019893 Wijesurendra, R. S., & Casadei, B. (2019). Mechanisms of atrial fibrillation. Heart, 105(24), 1860-1867. http://dx.doi.org/10.1136/heartjnl-2018-314267 Vann, M. R. (May 10, 2013) The Sound of an Afib Heartbeat. Everyday Health. https://www.everydayhealth.com/heart-health/sound-of-afib-heartbeat.aspx
Listen to the article here:

When EMTs arrive on the scene of an emergency, they have to remember their ABCs. These are Airway, Breathing, and Circulation. The absolute top priority for any patient is to ensure they have an open airway to breathe, that air is entering the lungs, and that the heart is pumping blood to the brain and other organs. This is also the most important thing our body does in daily life as well. We can go weeks without food, days without water, hours without ice cream, and minutes without oxygen. In order to get oxygen from the lungs to our brain and organs, we rely on one of the most remarkable organs in our body: the heart. The heart pumps automatically, nonstop, 24/7, from womb to grave. It consists of four chambers, two on top, and two on the bottom. Each heartbeat pulls blood into the top two chambers and pumps it out of the bottom two. The bottom two are more muscular and do the heavy lifting. Unfortunately, the heart can deteriorate and lead to heart failure. Heart failure is a condition where the heart can’t pump well enough to deliver oxygen to the organs effectively. The heart is still pumping, but organs are not receiving enough oxygen to function. This is not good. Heart failure affects over six million Americans and ten times as many people worldwide. Risk factors for heart failure include: Heart failure has several signs and symptoms. Some of the most consistent are edema and shortness of breath. Edema is fluid trapped in the body’s tissues and most often pools in the lower extremities and the abdomen. Shortness of breath is due to the heart failing to deliver enough oxygen. This is particularly prevalent when trying to do activities or when lying down. Shortness of breath can keep patients from exercising or sleeping, which only exacerbates problems. Patients who have limited exercise in their routine may not be aware of progressive difficulty, masking this important symptom. Other symptoms can be broad and nonspecific. They include: If you have heart failure and find yourself experiencing several of these conditions simultaneously, especially with edema and shortness of breath, we urge you to contact your physician immediately. Additionally, you may want to keep track of your level of fatigue because this symptom increases as the heart failure progresses. The excellent news is that new and exciting monitoring devices are currently being developed to help patients manage their heart failure and determine if their condition is deteriorating. Check out clinical research options available to you with ENCORE Research Group on our enrolling studies page. By Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Albert, N., Trochelman, K., Li, J., & Lin, S. (2010). Signs and symptoms of heart failure: are you asking the right questions?. American Journal of Critical Care, 19(5), 443-452. https://doi.org/ajcc2009314 Groenewegen, A., Rutten, F. H., Mosterd, A., & Hoes, A. W. (2020). Epidemiology of heart failure. European journal of heart failure, 22(8), 1342-1356. https://doi.org/10.1002/ejhf.1858 U.S. Department of Health & Human Services/Centers for Disease Control and Prevention (October 14, 2022). Heart failure https://www.cdc.gov/heartdisease/heart_failure.htm
Listen to the article here:
Heart failure is quite frankly, a terrifying sounding condition. It is severe, but not as immediately drastic as it sounds. Put simply, heart failure is when the heart fails to pump as much blood as the body will need long-term. The heart works like a balloon, filling with blood and contracting to pump it out. Ejection fraction is a term used to describe the amount of blood pumped out compared with the total the heart can hold. In a normal heart, 50-70% of blood is ejected with each heartbeat. When this amount falls below 40%, a person has a reduced Ejection Fraction (the rEF of HFrEF). This is a serious condition. The heart pumps blood to every cell in the body. This is how cells receive oxygen and nutrients, and how they get rid of waste products. Without enough blood, cells suffocate. Oxygen isn’t reaching cells and the brain interprets this as being short of breath. Common symptoms of HFrEF include: Inside the body, doctors can also look for diagnostic markers. These may include structural changes to the heart and increased natriuretic peptides. Natriuretic peptides are hormones that regulate the amount of salt and water in the blood. They act as vasodilators, opening blood vessels which can be helpful in compensating for heart failure. The body attempts to compensate for the loss of oxygen and nutrients in the blood in many ways, but long term the body has trouble sustaining with heart failure. Who is at risk of developing HFrEF? Unfortunately, it is more prevalent in the United States than almost anywhere else, affecting 6.5 million Americans each year. Risk factors include age, being male, obesity, and smoking. Additionally, other medical conditions increase your risk of developing Heart Failure with reduced Ejection Fraction. Previous heart attacks, coronary heart disease, diabetes, and hypertension are some associated conditions. All told, HFrEF leads to around a million hospitalizations every year, and being hospitalized for HFrEF comes with a low 5-year survival rate. What can be done? There are several methods of dealing with a reduced ejection fraction. Some methods treat symptoms, such as diuretics, and others can help reduce mortality, such as beta-blockers. There are several other medications and even some implantable devices that can help with HFrEF. These can help improve your ejection fraction or health outcomes but are not yet a silver bullet. New medications with increased outcomes and fewer side effects are entering clinical trials and may help with the underlying condition. To learn more about current heart failure research options, call our office today. Written by Benton Lowey-Ball, BS Behavioral Neuroscience
Bloom, M. W., Greenberg, B., Jaarsma, T., Januzzi, J. L., Lam, C. S., Maggioni, A. P., … & Butler, J. (2017). Heart failure with reduced ejection fraction. Nature reviews Disease primers, 3(1), 1-19. https://www.nature.com/articles/nrdp201758 Martinez-Rumayor, A., Richards, A. M., Burnett, J. C., & Januzzi Jr, J. L. (2008). Biology of the natriuretic peptides. The American journal of cardiology, 101(3), S3-S8. https://doi.org/10.1016/j.amjcard.2007.11.012 Murphy, S. P., Ibrahim, N. E., & Januzzi, J. L. (2020). Heart failure with reduced ejection fraction: a review. Jama, 324(5), 488-504. https://doi.org/10.1001/jama.2020.10262
Listen to the article here:
If someone in your family had a heart attack or stroke before the age of 60, you could be at risk and might want to have your blood tested for this little-known hereditary risk factor, Lp(a). Cardiovascular disease remains the leading cause of death in the United States, even during the COVID-19 pandemic. Determining and reducing the risk factors for cardiovascular disease is critical. Lipoprotein(a), also called Lp(a), pronounced “LP Little a” is a particularly dangerous culprit. Its levels are controlled by a single gene, and a single genetic variation in this gene is enough to drastically change Lp(a) levels. Unfortunately, since it is genetically determined, diet, exercise, and lifestyle have little or no effect on Lp(a) levels. High Lp(a) can contribute to several cardiovascular conditions. These include a two to three times increase in the risk of developing: Lp(a) has been referred to as the evil twin of the more familiar LDL (bad) cholesterol and is a triple threat because it is: There are two methods of measuring Lp(a). The most common method of measuring Lp(a) is by mass, in mg/dL. Measuring how many individual particles, regardless of size, is another method and is measured in nmol/L. It is important to know which method was used when understanding your numbers. If you have never had your Lp(a) level checked, we offer Lp(a) testing to our ENCORE community for those who pre-qualify (call for details). Currently, there are no approved therapies to lower Lp(a) levels and reduce one’s risk. However, three exciting therapies are currently being studied in clinical trials at ENCORE Research Group sites across Florida. The good news is that because of clinical research and your involvement, we have new treatments for elevated Lp(a) on the horizon! Written by Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Kamstrup, P. R. (2021). Lipoprotein (a) and cardiovascular disease. Clinical chemistry, 67(1), 154-166. https://doi.org/10.1093/clinchem/hvaa247 Miksenas, H., Januzzi, J. L., & Natarajan, P. (2021). Lipoprotein (a) and cardiovascular diseases. JAMA, 326(4), 352-353. doi:10.1001/jama.2021.3632 Health.harvard.edu Amgenscience.com
Listen to the article here:

Hypertension is one of the most prevalent conditions on the planet. Scientists estimate that it affects 30-45% of adults, somewhere over a billion people! Hypertension is the chronic elevation of blood pressure. The CDC defines it as above 130 mmHg systolic or above 80 mmHg diastolic. For short periods of time, elevated blood pressure can be useful – for exercise, say. People can have high blood pressure for years without symptoms. For long periods of time, however, hypertension is deadly serious. Unfortunately, living with high blood pressure can lead to a host of problems. Hypertension can lead to heart attack and stroke, and damage to the heart, brain, kidneys, and even eyes! Everyone is at risk of high blood pressure. In America, men have a higher likelihood of hypertension. There are also differences in ethnicity and race, non-Hispanic Black or African American adults are at the highest risk. Unfortunately, even the lowest risk categories still have around a 40% prevalence of high blood pressure. Clearly this is a large issue in America and around the world. The big culprit behind hypertension is the Renin–angiotensin–aldosterone system (RAAS). RAAS is a critical system for maintaining blood pressure. It regulates two primary factors: the amount of blood and how constricted blood vessels are. It does this through the kidney, liver, and adrenal gland (just above the kidneys). In response to body signals, the kidneys release an enzyme to the liver. In response, the liver produces the hormone angiotensin I. Another enzyme, angiotensin-converting enzyme (ACE) converts this to angiotensin II, which goes to work. Angiotensin II has wide-ranging effects to increase sodium and water retention. It also causes blood vessels to constrict. Angiotensin II is very short-lived, only lasting 1-2 minutes. One of its many effects is to get the adrenal gland to produce aldosterone. Aldosterone has similar effects as angiotensin II, but instead of a few minutes, it takes hours or days to take effect. The end result is that two major hormones – one fast-acting and one slow-acting – cause high blood pressure. There are many medications available to fight hypertension. Most of these, such as diuretics or beta-blockers, have wide-ranging side effects. This is because they are system-wide, indiscriminate actors on the body. Beta-blockers, for instance, slow the heart. This is helpful in lowering blood pressure but obviously leads to other effects on the body. RAAS-acting specific medications may be more helpful in combating hypertension with minimal side effects. ACE inhibitors, for instance, stop the fast-acting angiotensin II from having its effect on the body. This targeted approach to hypertension can lead to fewer side effects in some patients. Unfortunately, by acting on only the fast-acting portion of RAAS, they must be taken daily. Even worse, a few missed doses can have longer-term effects on blood pressure. Luckily, researchers are investigating other targeted methods of reducing the effect of RAAS, and blood pressure! Keep an eye out for a clinical research study to help investigate this exciting part of the fight against hypertension. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Sources Fountain, J. H., & Lappin, S. L. (2017). Physiology, renin angiotensin system. National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention. (September 27, 2027). Facts about hypertension. U.S. Department of Health and Human Services. https://www.cdc.gov/bloodpressure/facts.htm
Listen to the article here:
Heart disease is the leading cause of death in the United States. Though there are several types of heart disease, one of the main ways the heart actually dies is through congestive heart failure, when the heart fails to pump effectively. Ineffective pumping causes blood and other fluids to build up throughout the body. Eventually, the fluid buildup may keep the heart from functioning at all, a condition called acute decompensated heart failure. This is an emergency condition, and without rapid medical treatment quickly leads to death. Fortunately, with early intervention, several patients can recover – at least temporarily. Clearly, one of the keys to saving people is early intervention. The vocal cords and lungs may be affected by congestive heart failure. As these fill with fluid, there are changes in how the voice sounds. These changes are difficult for people to hear, but technology might be able to help out. One type of technology looking to tackle the topic is a deep neural network called HearO. Deep neural networks are a subset of artificial intelligence. These systems learn how to make predictions from examples. The HearO system, made by the company Cardio Medical, analyzed the voices of people with congestive heart failure. The system learned by comparing people’s voices while they were “wet” (fluid-filled while in the hospital) and “dry” (after hospital treatment and discharge). Using this, the system learned to detect voice differences in the severity of the condition. The HearO system has now been packaged as a smartphone app. Patients talk into the app every day and it compares their voice to itself. It scans for changes that indicate a fluid build-up (and danger!). The hope is that HearO will help detect changes in the voice before acute decompensated heart failure occurs. Clinical trials are currently underway to test the HearO’s effectiveness and some of our ENCORE Research Group sites are enrolling for this. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Sources: Amir, O., Abraham, W. T., Azzam, Z. S., Berger, G., Anker, S. D., Pinney, S. P., … & Edelman, E. R. (2022). Remote speech analysis in the evaluation of hospitalized patients with acute decompensated heart failure. Heart Failure, 10(1), 41-49. Brooks, M. (2015, December 15). Smartphone app could give voice to congestion in heart failure. Medscape. https://www.cordio-med.com/wp-content/uploads/2021/12/smartphone-app-could-give-voice-to-congestionin-heart-failure.pdf Tomov, N. S., & Tomov, S. (2018). On deep neural networks for detecting heart disease. arXiv preprint arXiv:1808.07168.

Healthy eating and exercise can help with not only your waistline but also cardiometabolic health. Carrying around extra fat can negatively affect your whole body; some areas of concern include the liver, heart, and joints. Although many people can maintain a healthy diet and exercise routine to keep the weight off, some folks need extra help with medication.
The liver is the largest organ inside your body and is integral in filtering harmful substances from your blood. When too much fat builds up in your liver, this is called fatty liver disease. This can progress to damaging and scarring of the liver. The scaring can ultimately lead to liver failure. Lifestyle changes, like healthy eating and exercise, are currently the only treatments for fatty liver disease, although many clinical trials are currently looking for a safe and effective therapy.
Heart disease remains the world’s leading killer. While extra fat itself does not directly cause heart attacks, it leads to other causes that can. High cholesterol, high blood pressure, and diabetes are among those that build up plaque in the arteries leading to heart attacks. ENCORE Research Group offices have many clinical trials in these areas!
Being overweight can affect your joints by raising your risk of developing osteoarthritis. The extra weight puts additional stress on your weight-bearing joints, such as your knees, which can cause additional wear and tear. Additionally, inflammation associated with weight gain might contribute to problems in other joints such as the hands.
For the folks who need more than just a healthy diet and exercise to help with medical conditions, the good news is that many new cutting-edge treatments are being studied and are available to you. Call your local ENCORE Research Group office today to get involved in our research trials.
Sources:
heathline.com
health.clevelandclinic.org
health.harvard.edu

How Do You Know If You Have High Blood Pressure?
The truth is, you don’t. The only way to really know if you have high blood pressure is by getting your blood pressure checked regularly. High blood pressure or hypertension (HTN) is known as the “silent killer” because it causes sudden heart attacks or strokes resulting in serious injury or possibly death with no warning.
The Effects of Hypertension
HTN causes more than just heart attacks and strokes. Prolonged HTN can cause serious illnesses such as:
- Kidney Disease — HTN may cause damage to the arteries surrounding the kidney. The damage can affect the kidney’s ability to filter blood efficiently.
- Heart failure — Heart failure occurs when the heart has to work harder to supply blood to the body, and HTN can cause extra work for the heart.
- Loss of Vision — HTN can strain or damage blood vessels in the eyes.
- Sexual Dysfunction — HTN can lead to erectile dysfunction in men or lower libido in women.
- Angina — Over time, HTN can lead to heart disease or microvascular disease (MVD). Angina, or chest pain, is a common symptom.
- Peripheral artery disease (PAD) — Atherosclerosis caused by high blood pressure can cause a narrowing of arteries in the legs, arms, stomach, and head, causing pain or fatigue.
How to Prevent a Visit from the “Silent Killer.”
One way to decrease your risk of heart disease from HTN is to know your numbers. Below is a chart from the American Heart Association that accurately details healthy vs. unhealthy blood pressure numbers.
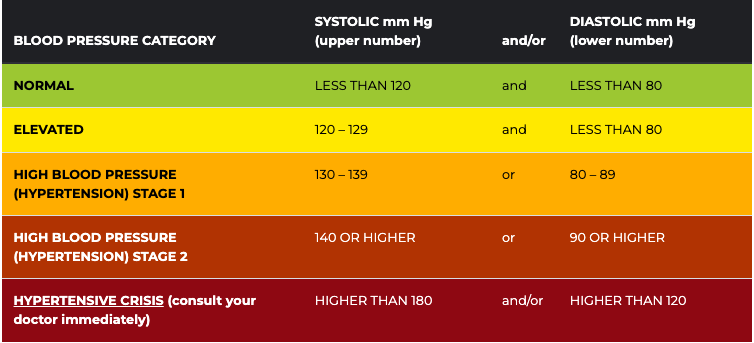
The second way is to be aware of your risk.
There are many risk factors for HTN and being aware of them can give you the knowledge to make healthy changes.
- Diet — Diet plays a considerable role in elevated blood pressure levels. Diets high in salty, fatty, and processed food increase your blood pressure, causing HTN. A good diet would be one that is high in vegetables, fruits, and lean meats.
- Physical Activity — Regular physical activity improves blood circulation and decreases your risk for HTN.
- Alcohol and tobacco use — Excessive alcohol and tobacco use can cause HTN and increase your risk of heart attack, stroke, and heart disease.
Other risk factors that you need to be aware of but are out of your control are:
- Family history
- Age
- Gender
- Race
Overcome Hypertension
How can you overcome hypertension? One way is to talk with your doctor about any medications or specific lifestyle changes you can make to reduce your risk. Another way is to participate in clinical trials. Clinical trials are a great tool to get to know your health more, receive one-on-one quality attention from a medical professional, and access to the latest therapies that are not currently on the market. ENCORE Research Group is currently enrolling in studies for hypertension. If you or someone you know would like to participate, please call 904-730-0166 or visit encoredocs.com.
Everyone should know these important signs.
Click play below to watch an informative video by the American Heart Association.
In 2020 heart disease killed twice as many people as COVID-19 in the United States.1 Some may find this surprising due to the lack of news coverage on heart disease. Historically heart disease has always been one of America’s most serious epidemics. It has been a leading cause of death since the turn of the 20th Century. Following World War II, the National Heart, Lung and Blood Institute began a long-term study known as the Framingham study to identify the cause of heart disease. The Framingham study is an enormous observational study in Framingham, Massachusetts. Researchers conducted physical examinations on participants every two years to study contributing factors to heart disease and are now on their 3rd generation of participants. The Framingham study identified many currently known risk factors, such as high blood pressure and high cholesterol. Researchers began developing medications to combat cholesterol levels once high cholesterol was identified as a significant risk factor. Some of our most exciting research at ENCORE Research Group is for new cholesterol-lowering medications such as Antisense Oligonucleotides (ASOs), Small Interfering RNA (siRNAs), and Adnectins. Antisense oligonucleotides (ASOs) are short, synthetic single-stranded fragments of RNA that can reduce, restore, or modify protein expression. ASOs have been designed specifically to target high levels of LDL (bad cholesterol) in the bloodstream in a different way than current medications. They are also being studied to reduce lipoprotein a [Lp (a) or “Lp little a”] in patients with elevated levels by targeting a building block of the Lp(a). Small interfering RNA (siRNAs) are another type of RNA therapy that is being used in clinical trials to reduce the risks of cardiovascular disease. Unlike ASOs which are single-stranded oligodeoxynucleotides, siRNAs are double-stranded RNA molecules. SiRNAs are used in the silencing of disease-causing genes for the treatment of atherosclerotic cardiovascular diseases. Adnectins are a class of drugs used to target proteins. Adnectins can be rapidly developed to bind proteins or other necessary targets. Currently, adnectins are being used in clinical trials to bind with a human protein called PCSK9. This binding blocks the interactions between PCSK9 and LDL (bad cholesterol) receptors. As a result, the levels of LDL cholesterol in the body are lowered. We are optimistic about these new technologies; they may give us the arsenal to fight back against heart disease. If you have high cholesterol levels that are not being adequately managed by your current medications, we may be able to help you get involved in a research study that may help get you back on track! As many of our readers know, most research studies offer access to cutting-edge therapies at no cost to patients. Call us to find out how you can get involved today! [1] CDC, https://www.cdc.gov/nchs/products/databriefs/db427.htm
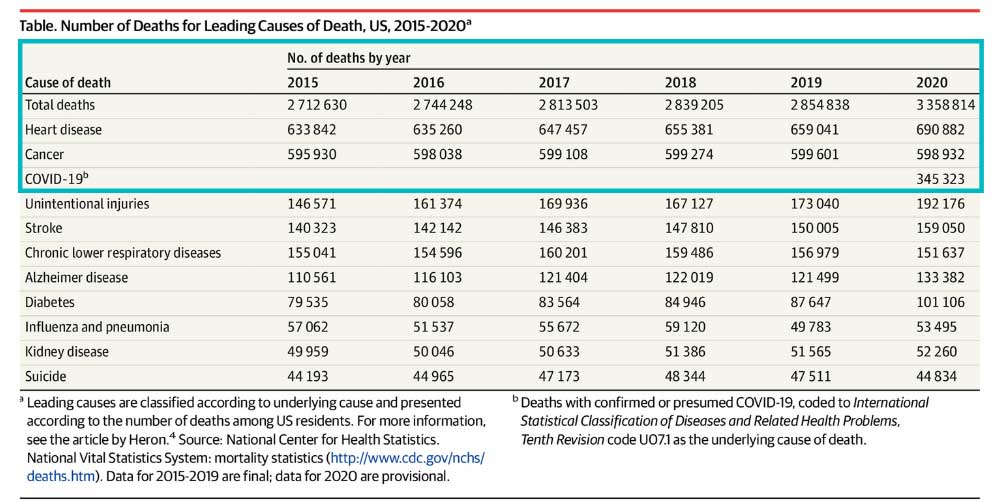
5 Things to Know about Lp(a) Lipoprotein(a), or Lp(a), is an independent risk factor for atherosclerotic cardiovascular disease. Cardiovascular disease is the leading cause of death in both men and women in the US and globally . You may have heard of LDL cholesterol, or “bad cholesterol,” as a risk factor for heart disease, but Lp(a) can be just as dangerous. Lp(a) flies under the radar of many physicians. This is because the awareness of Lp(a) is still very low, very little is understood about the protein and the treatment options are limited. What is LP(a)? Lp(a), pronounced “LP little a,” is a protein that is attached to LDL cholesterol. It is composed of an LDL-like particle, but it has a second protein coiled around it. Recent studies have shown that people born with elevated Lp(a) can be two to four times as likely to have a heart attack or serious cardiac related risk. Lp(a) is present in 20% of the population. What differentiates LP(a) from other heart disease risk factors? LP(a) is so unique because it is a completely genetic risk factor. Meaning, having an elevated LP(a) is almost entirely determined by the genes you inherit. There is no evidence that a healthy lifestyle will lower your Lp(a). However, that does not mean those with high levels shouldn’t practice healthy habits. Reducing other risk factors that are determined by quality of health can still reduce the overall risk of heart disease. Another risk factor that sets LP(a) apart is that it is an independent risk factor. It has been linked to heart disease in younger adults who are otherwise healthy and have no prior cardiovascular risks. Elevated LP(a) has affected the lives of many who are otherwise healthy. For example, Tennis legend Arthur Ashe, who had his first heart attack at age 36. Bob Harper, a celebrity fitness trainer was also affected and nearly died of a heart attack at age 52. Who should be tested for Lp(a)? Studies show that there is a higher risk of a cardiovascular event if Lp(a) levels start to rise above 30 mg/dl. There is an even greater risk at levels 50 mg/dl and higher. There are an estimated one in seven people at or above this threshold. If you’ve had a cardiac event but your cholesterol levels are normal, or you have a family member with heart disease at an early age, have a cardiovascular event despite normal lipid levels, have a family history of Lp(a), or have aortic valvular disease at an early age then you should get tested for Lp(a). As mentioned, Lp(a) is a genetically mediated risk factor. “This means it runs in families,” Albert Lopez, MD, DO, FASPC, internal physician and lipid specialist in Jacksonville, FL says. “Those individuals that have it, you have a 50% chance of giving to your children.” Dr. Lopez believes there should be cascade screening, meaning asking family members if they have it and then getting tested. No FDA approved remedies for Lp(a) Currently there are no FDA approved remedies for elevated Lp(a). Statins, a widely known and used therapy that lowers LDL cholesterol does not reduce Lp(a) and has been shown to sometimes result in a slight increase. One therapy that has been shown to work is asphersis. This process filters a patient’s blood by circulating it through a machine and removing Lp(a) particles. However, this process is reserved for high-risk patients because it is extremely expensive, requires weekly visits and involves risks. After stopping apheresis, the Lp(a) levels begin to rise again. New Advancements in Science regarding Lp(a) Luckily, there are new drugs on the horizon that could potentially help those suffering from elevated Lp(a) levels. “What is exciting is that we are in totally nerd, sci-fi treatments now,” Dr. Lopez says. “We can actually stop your genes from making this protein by using a little snip that crinkles it up and doesnt let it read.” In other words, new studies are using gene silencing techniques to achieve a large and durable reduction of Lp(a). These therapies and medicines are still in clinical trials now. ENCORE Research group is conducting research studies for people with elevated Lp(a) in hopes to find a drug that will lower Lp(a) levels. It is up to the public to participate in these research studies to help those suffering from elevated Lp(a) levels.

For some patients, managing cholesterol creates a challenge. Statins are a safe and standard treatment but many people have very high levels of cholesterol that require more than statin drugs alone. Others cannot easily tolerate statins. Nonetheless, treating cholesterol saves lives and avoids heart attacks and strokes. Thankfully, the future is here with new breakthroughs that can change the way we maintain healthy cholesterol levels due to continued research and clinical trial participants. We outline some of these exciting technologies below. Antisense oligonucleotides (ASOs) are short, synthetic single stranded fragments of RNA that can reduce, restore or modify protein expression. ASOs have been designed specifically to target high levels of LDL (bad cholesterol) in the bloodstream in a different way than current medications. Firstly, ASOs targets the source of the disease resulting in a higher chance of success compared to therapies targeting downstream pathways. Secondly, ASOs are not metabolized by cytochrome P450 as most other drugs are. This significantly reduces the chance of one drug interacting with another drug in the body which could potentially cause more harm than good. Small interfering RNA (SiRNAs) are another type of RNA therapy that is being used in clinical trials to reduce the risks of cardiovascular disease. Unlike ASOs which are single-stranded oligodeoxynucleotides, siRNAs are double-stranded RNA molecules. SiRNAs are used in the silencing of disease-causing genes, in this case the genes involved in creating cardiovascular diseases, and it has made great progress. Adnectins are a class of drugs used to target proteins. Adnectins can be rapidly developed to bind proteins or other necessary targets. Currently, adnectins are being used in clinical trials to bind with a human protein called PCSK9. This binding blocks the interactions between PCSK9 and LDL (bad cholesterol) receptors. As a result, the levels of LDL cholesterol in the body are lowered. These technologies hold the potential to not only better manage cholesterol levels and thereby reducing heart attack and stroke risk, but many other conditions as well. Source: US National Library of Medicine
National Institutes of Health
The old saying goes: Men are from Mars and Women are from Venus. This exaggeration is- well… an exaggeration, but there are some differences between male and female heart health that causes an inkling of truth to shine out through the expression. The most common kind of heart disease, among both men and women, is coronary artery disease. Coronary artery disease is caused when cholesterol plaque is built up inside the arteries, and if left untreated coronary artery disease can obstruct blood flow to the heart muscle and lead to a heart attack.
When experiencing a heart attack, the individual will usually experience chest pain, shortness of breath, and pain in their left arm, but these symptoms are not universal. Remember when we were talking about the differences between men and women? Women are more likely to experience uncommon heart attack symptoms than men are! These symptoms can include indigestion, pain in both arms, unusual fatigue and abdominal discomfort. Physicians are still uncertain why women are more likely to experience unusual symptoms. There are some theories about hormonal changes and the difference in valve and vessel sizes, but for the most part it is still unknown.
Lowering your risk of a heart attack, however, is not a mystery. Research shows staying active, eating healthy, and monitoring your blood pressure and cholesterol levels regularly leads to decreased cardiovascular risk. Research also shows that individuals involved in clinical research have better health care outcomes than those who are not.
We are currently enrolling in studies that may help you lower important factors like elevated triglycerides and cholesterol which may help lower your risk of cardiovascular events.
References:
https://www.hopkinsmedicine.org/heart_vascular_institute/centers_excellence/womens_cardiovascular_health_center/patient_information/health_topics/menopause_cardiovascular_system.html
https://www.lahey.org/article/differences-between-mens-and-womens-hearts/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3018605/
https://www.clinicaltrials.gov

What causes a heart attack?
A heart attack (myocardial infarction) means that blood flow to the heart muscle has been decreased enough to cause damage to the heart muscle. Some causes of blocked blood flow include blood clots, cholesterol build up, and rupture of plaque within the blood vessel. For those who have already suffered a heart attack, it is important to reduce the risk of recurrent attacks. Research has shown that there are several steps that can be taken to help reduce the risk of recurrent heart attacks.
Proven things you can do to prevent heart attacks
- Lower cholesterol
- Lower triglycerides
- Lower blood pressure
- Stop smoking and avoid secondhand smoke
- Eat fish
- Increase physical activity as allowed by your doctor. Inactive people have nearly twice the risk of heart disease as those who are active.
- Talk with your doctor about medicines that can decrease blood clotting
Medications that can reduce risk of heart attack
- Cholesterol lowering medication, which include statins and non-statins
- Triglyceride lowering medications
- Medications that decrease inflammation
Current research is underway to study improving health after a heart attack
- Weight loss: Heart attack is three times higher in those who are obese than in those who are lean.
- New medications for those with unique cholesterol metabolizing problems.
- Anti-inflammatory medications targeting inflammation in blood vessels.
At ENCORE Research Group we have clinical research studies for many of the risk factors mentioned above. Participating in a research study can help keep you motivated on your journey to better health. If you are interested in participating in any of our research studies, call your local office today!
The heart is vital (literally), so it’s important to keep it in tip-top shape! The rest of the body depends on the heart to deliver blood and oxygen to all its cells and organs. If the heart becomes damaged, it can lead to what is known as heart failure. Keeping your heart healthy not only involves proper diet and exercise, but also involves making sure conditions that can cause heart damage are properly managed.
Some conditions that can damage the heart are:
- cardiomyopathy
- coronary artery disease
- diabetes
- heart attacks
- high blood pressure
During heart failure the heart is unable to pump blood effectively enough to meet the body’s demands. Because the heart cannot fulfill its primary duty, it will try to compensate by enlarging itself, increasing muscle mass or pumping faster. The body can also react by narrowing blood vessels and diverting blood away from less important tissues and organs. As heart failure worsens the compensations and symptoms begin to show.
Common symptoms of heart failure include: shortness of breath, fatigue, coughing, racing heart, excessive tiredness, loss of appetite, and chest pain. Risk factors for developing heart failure include diabetes, poorly controlled high blood pressure, high cholesterol, or family history of heart failure. If you think you might have symptoms of heart failure, it’s important to speak with your doctor as soon as possible.
There are about 5.7 million adults in the United States who have heart failure and it’s the leading cause of death in diabetics. In most cases, heart failure cannot be reversed once diagnosed. However, researchers are continuing to study ways to reverse heart failure as well as new and better ways to treat it. Currently, many of our ENCORE research sites have new heart failure research studies enrolling. If you or someone you know has heart failure, and are interested in participating, call our office to find out more!

Three New Breakthroughs in Heart Disease
Heart Disease is a general term for heart conditions that negatively impact the heart’s ability to perform its vital functions. On average 1 in 4 American deaths each year are due to heart disease. Fortunately, each year new discoveries are made that allow us to treat heart disease more successfully. Here are three of the latest discoveries.
- Dialysis for Heart Failure?
One of the symptoms of heart failure is fluid retention, which can lead to kidney
problems. Diuretics are currently the standard treatment for fluid retention, however there is a new treatment where a catheter in inserted through the neck so that it surrounds a major lymphatic vessel. The excess fluid is removed from the lymphatic system and then pumped back into the circulatory system where it is removed by the kidneys. This new treatment avoids some of the negative side effects of oral diuretics such as low blood pressure and decreased kidney function.
2. Beta Blockers: Old dog, new tricks?
A new study at York University in Toronto has analyzed the effect of beta blockers on
coronary gene expression in patients with heart failure. Researchers found that beta blockers “largely reverse the pathological pattern of gene expression observed in heart failure.” More research is needed to determine whether beta blockers can be used to protect against heart failure.
3. Tick saliva saving lives?
While ticks are often the subject of nightmares researchers now believe they can lead to a dream solution for myocarditis, heart attack and stroke. Ticks use proteins called ‘evasins’ to escape their host’s detection by blocking the host’s inflammatory response. Researchers are now isolating these evasins in a ‘bug to drug’ formula. Hopefully these drugs will be able treat a variety of inflammatory diseases.
At ENCORE Research Group we conduct cutting edge research similar to those seen above. While we do not have any ‘bug to drug’ studies at this time, we do have a heart failure study involving a new use for an already FDA approved medication. If you are interested in learning more about our current studies visit our “Enrolling Studies” tab at the top of the page.

If you have high cholesterol you may dread going to your doctor, especially if they are going to complete a cholesterol blood test. You know they prescribed a statin, but the muscle cramping you experience after taking it just isn’t worth it. How do you tell your doctor that the medication they prescribed just isn’t working for you? You are not alone, and there are options available for you.
We all know that having excess cholesterol in our blood is a bad thing, but why is it so bad? High cholesterol has often been called ‘The Silent Killer’. In fact, according to the CDC heart disease is responsible for 1 in 4 American deaths every year.[1] High cholesterol is known to cause plaque formation in arteries, constricting blood flow to vital organs in your body. Even worse, cholesterol plaques can become dislodged from the walls of the arteries potentially causing blood clots. Both heart attacks and strokes can be caused by plaques reaching the heart or brain respectively. If lifestyle changes such as a good diet and exercise can’t bring down your cholesterol numbers, you may need a medication. The most common cholesterol lowering medications to date are statins such as Crestor, Lipitor, or Zocor. These medicines have been life saving for many people that can tolerate them. However, some people are intolerant to statins and will experience side effects such as painful muscle cramps, inflammation and more.
If you are allergic to or can’t handle statins what can you do? It is crucial to keep your cholesterol levels down, lowering your risk for a heart attack and stroke. You may try one of the medications already on the market for people with statin intolerance such as Zetia, Juxtapid and Repatha. However, each of these drugs have their own risks. Zetia can cause symptoms similar to those caused by statins. Juxtapid, a newer medication, has been found to significantly reduce LDL bad cholesterol by 40-50%. Sadly, it also caused diarrhea, nausea, vomiting or abdominal pain in 28% of patients.[2] In 2015 the FDA approved Repatha, a new class of drug called a PCSK9 inhibitor that is very successful in lowering LDL. Unfortunately, due to the cost of development and production the annual cost is around $14,000 dollars making it unaffordable for most people.
If you’ve had trouble taking statins in the past you may be asking “what do I do now”? Many of our participants are looking for alternative treatments or want to be part of cutting edge research. I encourage you to check out the cholesterol research studies we are conducting at many of our research centers. You may qualify for a new oral medication or to receive PCSK9 in an upcoming study! The medicines being researched for people who cannot take statins may significantly alter the future of cardiovascular disease. We need your help to bring these new medications to market!
References:
[1] “Heart Disease Fact Sheet.” Centers for Disease Control and Prevention. Centers for Disease Control and Prevention, 16 June 2016. Web. 27 Apr. 2017.
[2] Orrange, Sharon, MD. “Finally, a Non-Statin Cholesterol Medication That Works: Introducing Juxtapid.” The GoodRx Prescription Savings Blog. N.p., 06 June 2014. Web. 27 Apr. 2017.