GRID VIEW
Diabetes is a widespread disease where the body cannot process sugars effectively. It has myriad effects on the body, including in the gut. Diabetes affects nearly every part of the gastrointestinal tract, from the throat to the anus. Diabetes is one of the most common causes of a condition called gastroparesis. Gastroparesis is from the Greek language. Gastro- means “stomach,” –paresis indicates a partial paralysis, so gastroparesis means a partial paralysis of the stomach; it empties food slowly. This condition is more likely to affect women than men, but there aren’t good numbers on how many people it affects in total. Symptoms of diabetes and gastroparesis may overlap but include feeling full, weight changes, nausea, vomiting, bloating, and diarrhea. Gastroparesis can lead to serious complications like malnutrition, decreased quality of life – including anxiety and depression, and significantly higher mortality. The effects of diabetes further exacerbate these complications. How diabetes actually affects stomach muscles is complex and fascinating. The digestive tract is lined with smooth muscle. Smooth muscle isn’t connected to bone and contracts in long, slow, low-energy waves. This is great for contracting blood vessels or moving food through the stomach and intestines. These are involuntary muscles, meaning we can’t consciously control them. In fact, the brain modulates the activity of gastrointestinal muscle, but it’s controlled by our “little brain” in the intestines! This little brain is made of around 500 million neurons and is called the enteric nervous system. The enteric nervous system is a distributed brain-like bunch of neurons and other cells spread throughout our abdomen that may be able to act independently of our big brain. It is responsible for getting the smooth muscle to contract rhythmically and in response to food. The enteric nervous system also includes cells that aren’t neurons. An important type is interstitial cells of Cajal (kuh-jaal). These are pacemaker cells that regularly generate electrical signals to coordinate muscle. The prominent players in the enteric nervous system, however, are neurons. Though neurons are electric, they communicate with other neurons by releasing neurotransmitters and receiving them in specialized receptors. These are often the same neurotransmitters we find in the brain, though they may have different functions. Dopamine is a great example. In the brain, dopamine receptors are part of the reward pathway, giving you feelings of pleasure and motivation. In the enteric nervous system, dopamine receptors act to suppress muscle movement. More dopamine in the brain makes you feel happy, but more dopamine in the gut restricts the movement of food. In diabetes, this can get all messed up. A key aspect of uncontrolled diabetes is the inability of the body to regulate blood sugar. This causes a few significant disturbances. Primary among these is neuron damage. Since the affected neurons are involuntary, we call this autonomic neuropathy. Autonomic neuropathy in the gastrointestinal tract can take the form of fewer neurons and ones that can’t communicate well because of damage. Diabetes can also lead to changes in the signaling pathways of smooth muscle and may destroy some of the pacemaking interstitial cells of Cajal. Together, these changes result in fewer smooth muscle contractions and a slower flow of food through the stomach and intestinal tract. The slow flow of food in gastroparesis can cause a feedback loop. Slow food is more likely to be mistaken for invaders, potentially causing inflammation. Even worse, the extra time in the digestive tract means there is more time for glucose, a major sugar, to get absorbed – increasing blood sugar and making the symptoms of diabetes worse. So, what can be done with diabetic gastroparesis? The first step is lifestyle alteration. Smaller and more frequent meals may help alleviate symptoms. Increasing noncarbonated liquids and decreasing fat and fiber may also help. Monitoring nutrient levels and electrolytes is critical. Beyond this, few medications are currently available. The most prominent are dopamine D2 receptor antagonists; meaning they inhibit the effect of dopamine. Metoclopramide (meh-tow-klow-pruh-mide) inhibits dopamine and mimics serotonin. It is effective at increasing the speed of emptying. It can cross the blood-brain barrier, however, causing unintended side effects in the brain. Domperidone (daam-peh-ruh-down) is another dopamine receptor antagonist. It doesn’t cross into the brain but can affect the heart, slowing the time it takes to recharge between beats. This medication is not approved in the United States, though it’s been approved in several other countries for decades. Clinical research is currently looking into new medications that may provide the same dopamine receptor inhibition as metoclopramide and domperidone but without the ability to affect the brain or heart! With the help of clinical volunteers, diabetic gastroparesis may pass quicker than we expected! At the time of writing this article, clinical research for diabetic gastroparesis is enrolling at our Nature Coast Clinical Research – Inverness office. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Aswath, G. S., Foris, L. A., Ashwath, A. K., & Patel, K. (2017). Diabetic Gastroparesis. https://www.ncbi.nlm.nih.gov/books/NBK430794/ Bharucha, A. E., Kudva, Y. C., & Prichard, D. O. (2019). Diabetic gastroparesis. Endocrine reviews, 40(5), 1318-1352. https://academic.oup.com/edrv/article/40/5/1318/5487986?login=true Isola, S., Hussain, A., Dua, A., Singh, K., & Adams, N. (2018). Metoclopramide. https://www.ncbi.nlm.nih.gov/books/NBK519517/ Puoti, M. G., Assa, A., Benninga, M., Broekaert, I. J., Carpi, F. J. M., Saccomani, M. D., … & Borrelli, O. (2023). Drugs in focus: Domperidone. Journal of pediatric gastroenterology and nutrition, 77(2), e13-e22. DOI: 10.1097/MPG.0000000000003822 Sanders, K. M., Koh, S. D., Ro, S., & Ward, S. M. (2012). Regulation of gastrointestinal motility—insights from smooth muscle biology. Nature reviews Gastroenterology & hepatology, 9(11), 633-645. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4793911/ Sugumar, A., Singh, A., & Pasricha, P. J. (2008). A systematic review of the efficacy of domperidone for the treatment of diabetic gastroparesis. Clinical gastroenterology and hepatology, 6(7), 726-733. https://www.cghjournal.org/article/S1542-3565(08)00241-3/fulltext Tonini, M., Cipollina, L., Poluzzi, E., Crema, F., Corazza, G. R., & De Ponti, F. (2004). Clinical implications of enteric and central D2 receptor blockade by antidopaminergic gastrointestinal prokinetics. Alimentary pharmacology & therapeutics, 19(4), 379-390. doi: 10.1111/j.1365-2036.2004.01867.x Uranga-Ocio, J. A., Bastús-Díez, S., Delkáder-Palacios, D., García-Cristóbal, N., Leal-García, M. Á., & Abalo, R. (2015). Enteric neuropathy associated to diabetes mellitus. https://digital.csic.es/handle/10261/241840 Yarandi, S. S., & Srinivasan, S. (2014). Diabetic gastrointestinal motility disorders and the role of enteric nervous system: current status and future directions. Neurogastroenterology & Motility, 26(5), 611-624. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4104990/
Listen to the article here:
The immune system is awesome, but overwhelming. It’s filled with billions of cells and quintillions of proteins. There are neutrophils, dendritic cells, antibodies, B cells, macrophages, lymphoid cells, lymphocytes, the complement system, and more! Instead of trying to understand the whole thing, let’s narrow our focus down to just one type of cell, the T cell, and just one variant, T-helper 17, or Th17. T-cells are a type of white blood cell and are about the size of a red blood cell. They are adaptive, which means they change in response to threats. These cells start as virgin (or naïve) cells and transform into a specialized version when danger is detected. T-cells can be divided into two parts: killers and helpers. Killers are good at killing other (hopefully bad) cells, while helpers activate other cells and amplify immune responses. The cell we’re focusing on, Th17, is a type of helper cell, but a special one. Th17 was first identified in 2005, but scientists have rapidly learned loads about it. It is particularly good at helping the body fight unusual attackers like fungi and certain bacteria. When activated, it releases a powerful signaling chemical that increases inflammation and recruits other white blood cells, telling them to come and fight. In addition, it can assist in tightening the spaces between our border cells to keep invaders out. When the body detects unknown particles, cells release signaling molecules. When a T-helper cell encounters the right mix of these molecules, it transforms into the rallying Th17 captain which sounds the alarm. Unfortunately, all that shimmers is not silver. Th17 can certainly be useful in some circumstances, but it can be dangerous when activated by the wrong signals. In many of these cases, Th17 cells tell white blood cells to go nuts and attack anything that moves (or doesn’t move), but without a clear opponent, they just attack whatever’s around and cause an autoimmune response. Th17 has been implicated in diseases like experimental autoimmune encephalomyelitis (EAE), arthritis, and inflammatory bowel diseases (IBD) like Ulcerative Colitis. Let’s look at ulcerative colitis as an example. Ulcerative colitis is an inflammatory bowel disease where the immune system attacks benign bacteria or food particles. The causes aren’t clear, but part of the problem is a thinning of the mucus and separation of border cells that line the intestines. Many signaling molecules called interleukins (abbreviated IL-) are released in the disease state, including three important ones for Th17. These are IL-1β, IL-6, and IL-23 (write this down for the quiz at the end). The first two activate Th17, and that’s when IL-23 can turn it into a problem. In the presence of IL-23, Th17 sends wild signals and can cause the autoimmune problems listed above, including ulcerative colitis. Also, remember how Th17 helps tighten the spaces between border cells? It turns out that in the presence of IL-23 this function doesn’t work properly and the borders stay open, letting in more particles that the body attacks with inflammation. Scientists have been trying to find ways to solve the problems caused by Th17 since long before it was even known to exist. In the past, a treatment for something like ulcerative colitis might have been limited to restricting your diet. Currently, anti-inflammatory medications, steroids, and/or surgeries are used. Those are all big solutions bound to affect many other parts of the body and immune system. Now that Th17 has been identified as an occasional dirty traitor, researchers are instead targeting this specific cell to hopefully stop it from being activated incorrectly. With luck, we can help the T-helper cell to help us instead of unhelping us. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Kałużna, A., Olczyk, P., & Komosińska-Vassev, K. (2022). The role of innate and adaptive immune cells in the pathogenesis and development of the inflammatory response in ulcerative colitis. Journal of clinical medicine, 11(2), 400. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8780689/ Sender, R., Weiss, Y., Navon, Y., Milo, I., Azulay, N., Keren, L., … & Milo, R. (2023). The total mass, number, and distribution of immune cells in the human body. Proceedings of the National Academy of Sciences, 120(44), e2308511120. https://doi.org/10.1073/pnas.2308511120 Tesmer, L. A., Lundy, S. K., Sarkar, S., & Fox, D. A. (2008). Th17 cells in human disease. Immunological reviews, 223(1), 87-113. https://doi.org/10.1111/j.1600-065X.2008.00628.x Wu, B., & Wan, Y. (2020). Molecular control of pathogenic Th17 cells in autoimmune diseases. International immunopharmacology, 80, 106187. https://doi.org/10.1016/j.intimp.2020.106187
Scroll down to listen to this article.
Listen to the article here:

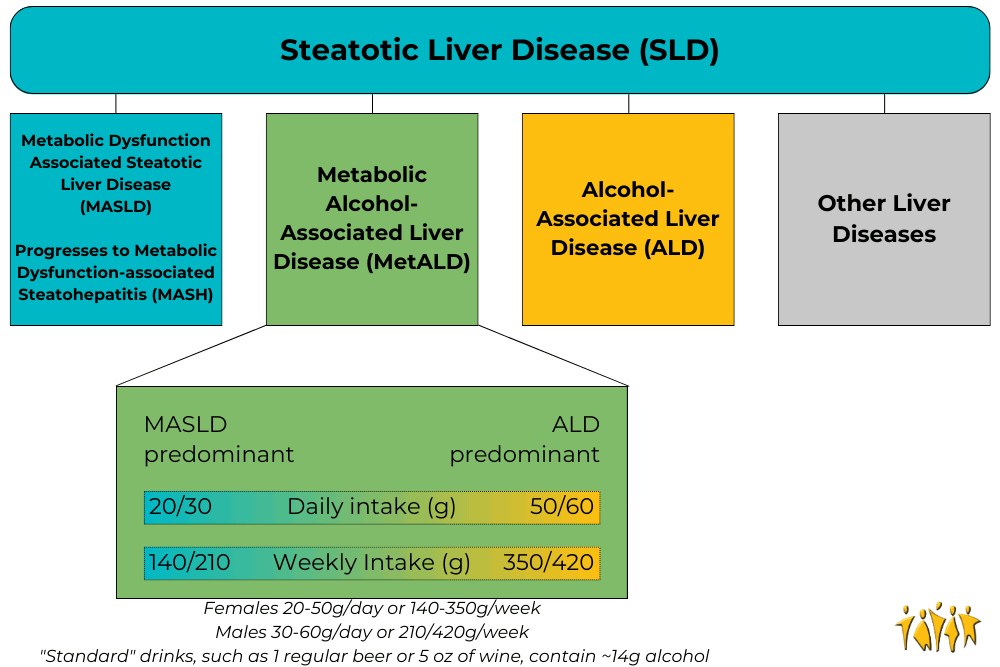
Medical terminology can be hard to understand. Much of it is in Latin, some is in Greek, several words are named after people, and terminology can change. Sometimes that change is a good thing, though. In June 2023 a collaboration of hundreds of experts in liver disease released new names for the liver diseases previously known as Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH).
Adapted from Rinella, M. E., et al., 2023
Under the broad category of Steatotic Liver Disease (SLD) we now have Metabolic dysfunction Associated Steatotic Liver Disease (MASLD), which can progress to Metabolic Dysfunction-Associated Steatohepatitis (MASH) and Metabolic Alcohol-associated Liver Disease (MetALD, which is MASLD and increased alcohol intake). This change was made for many reasons. The terms “non-alcoholic” and “fatty” may have been confusing, stigmatizing, or inaccurate. People who are not overweight may still have the disease, and those with the disease may still be consuming alcohol. Finally, naming a disease after what it isn’t (“nonalcoholic…”) is less than ideal. The new system describes the same symptoms but with more specific language. Steatosis is the accumulation of fat inside of cells and the disease is caused by changes in the metabolic system; how our cells change food into energy. A critical change has also been made with the adoption of the new term MetALD. MetALD describes people who have MASLD, but who still consume some alcohol. Alcohol affects the disease progression, but metabolic disruptions do as well. Hence, a term was developed to describe this overlap. These terms were planned and adopted by an international group of clinical researchers, scientists, educators, industry experts, and patient advocates. The American Association for the Study of Liver Disease (AASLD), European Association for the Study of the Liver (EASL), Asian Pacific Association for the Study of the Liver (APASL), and Asociación Latinoamericana para el Estudio del Hígado (ALEH) made up most of the participants and have ensured widespread adoption of the new terminology Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Rinella, M. E., Lazarus, J. V., Ratziu, V., Francque, S. M., Sanyal, A. J., Kanwal, F., … & NAFLD Nomenclature consensus group. (2023). A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Annals of Hepatology, 101133. https://doi.org/10.1097/HEP.0000000000000520
Scroll down to listen to this article.
Listen to the article here:
Nonalcoholic Steatohepatitis, or NASH, has no approved medications available for treatment. This isn’t because the disease is safe, however. NASH can lead to cell death, cells going rogue, collagen accumulation, fibrosis, cirrhosis, and liver cancer. One problem with treating NASH is that it is a multifactorial disease, meaning there are many possible causes that all lead to the same outcome. The current best methods for treating NASH are exercise, weight loss, and treating other conditions that may contribute. We will discuss scientifically backed information regarding these treatment options, but it is critical that any medical advice be discussed with your doctor. NASH has many many causes and affects a lot of body systems. Medical professionals that may be involved in NASH treatment include your primary care physician, a hepatologist, dietitian, endocrinologist, cardiologist, and others. Every person is an experiment of one, and your specific circumstances may contraindicate one or all of the methods discussed below. Talk to your doctor. Weight loss is the go-to method of treating NASH. A combination of diet and exercise is the best method to achieve weight loss. This ensures fewer calories enter the body than exit it, and that the body is burning weight from fat instead of from muscle. Losing weight very rapidly can be dangerous, so be conscientious of your body’s overall health (and speak with a professional!) Research has shown that reducing weight by as little as 5% (12.5 lbs for a 250 lb person) can help improve steatosis, the fat buildup in the liver. Losing 7% or more (17.5 lbs for a 250 lb person) also shows a reduction in inflammation and improved health of liver cells. When patients, particularly obese patients, lose 10% of their body weight (25 lbs for a 250 lb person) the structural liver changes known as fibrosis start to regress or stabilize. For NASH patients of a normal weight, they may see results when losing as little as 3-5% of body weight. Exercise is a great way to lose weight, but studies have shown that exercise can help your liver even when you aren’t losing weight. The exact mechanisms for how this works are complex and not fully known. Scientists have found that exercise helps make the body more sensitive to insulin – which helps it regulate blood sugar better. It can also help cellular metabolism. Exercise is associated with a reduction in the markers of liver inflammation and may help liver cells stay healthy. Aerobic exercise, also called “cardio,” is highly recommended. Resistance training, called strength training, is also helpful, especially if aerobics are not possible. NASH patients start seeing benefits when doing exercise for 150-300 minutes (2 ½ – 5 hours) per week of moderate intensity exercise or 75-150 minutes (1 ¼ – 2 ½ hours) per week of high intensity exercise. Always ease into a new exercise routine to avoid injury. Talking to a medical professional is also a good idea before starting new exercises (there is a theme to this article). Exercise burns calories, but to lose weight we also want to manage what calories we take in. Consult with your doctor or dietitian, but reducing caloric intake to around 500 fewer than the daily recommended value may help. Further, the number of calories is not directly correlated to the quality of the calories. NASH patients find improvements when reducing items that can damage the liver, including fructose and saturated fats. Fructose is a form of sugar that is often added to sugary beverages (usually in the form of high fructose corn syrup) and contributes to insulin resistance. Saturated fats are found in meats, including red meats and processed meats. As for specific diets, research is ongoing. The Mediterranean diet has the most research backing its success in NASH patients. It is rich in fruits, vegetables, whole grains, seafood, nuts, legumes, and olive oil. Other diets may be suitable as well, including intermittent fasting, ketogenic diet, and others. One recommendation is to take the Mediterranean diet and adjust it to fit you. Regardless of the diet choice, alcohol should be limited. For smokers and former smokers, alcohol should be eliminated entirely. It should go without saying that making major adjustments to your diet should be consulted with your doctor. Other than diet and exercise, treatments for NASH are all achieved by treating other conditions that contribute, and will vary depending on the individual. Conditions that contribute are obesity, diabetes, high blood pressure, high cholesterol, cardiovascular disease, and obstructive sleep apnea. Cardiovascular disease and obstructive sleep apnea are major contributors of mortality for NASH patients and should be taken seriously. Obviously these conditions are best treated by going to your doctor. NASH is a progressive disease that gets worse over time and leads to serious, occasionally deadly complications. Clinical trials may give us a medical NASH treatment in the future. Until then, give yourself a leg up (or liver) by consulting your doctor about treatments through diet, exercise, and underlying condition management. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: American Liver Foundation. (March 16, 2023). What are the treatments for NAFLD and NASH? NASH Treatment, https://liverfoundation.org/liver-diseases/fatty-liver-disease/nonalcoholic-steatohepatitis-nash/nash-treatment/ Van der Windt, D. J., Sud, V., Zhang, H., Tsung, A., & Huang, H. (2018). The effects of physical exercise on fatty liver disease. Gene Expression The Journal of Liver Research, 18(2), 89-101. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5954622/ Younossi, Z. M., Corey, K. E., & Lim, J. K. (2021). AGA clinical practice update on lifestyle modification using diet and exercise to achieve weight loss in the management of nonalcoholic fatty liver disease: expert review. Gastroenterology, 160(3), 912-918. https://doi.org/10.1053/j.gastro.2020.11.051
Scroll down to listen to this article.
Listen to the article here:
Is the liver the most amazing organ? Yes. It turns food into usable molecules. It makes proteins, bile, and hormones. It filters dangerous drugs and toxins. Without it, you would die within minutes. Also, the liver can regenerate (like a lizard’s tail!), which is basically magic. The liver is estimated to have over 500 individual functions and interacts with most body systems. In this article we’ll look at the liver, zooming in from basic facts to its cellular units. Then we’ll explore the functions of the liver. If you were to guess the largest organ in the body, would you guess the liver? I hope not, because it’s the skin. But the liver is in second place! It makes up around 2% of your body weight and usually contains about 10% of your blood. It’s located under the ribs, right below the diaphragm that inflates the lungs. It’s smooth and reddish brown when healthy (note: if you can see your liver’s color you are probably having a bad day). The liver can be divided into four parts called lobes and thousands of sub-parts called lobules. These are hexagonal columns of cells arranged so that blood can travel through carrying nutrients in and toxins and waste out. Four types of cells make up the liver: hepatocytes, epithelial cells, Kupffer cells, and stellate cells. Most of the liver is composed of hepatocytes. These are the workhorses of the liver. Hepatocytes convert fats (called lipids), sugars (called carbohydrates), and proteins (called proteins) into usable forms. They detoxify dangerous things and excrete bile and cholesterol. The barrier epithelial cells line the walls (including blood vessel walls) inside the liver and do some filtering of small particles. It is thought that these may also do some clearance of viruses. Kupffer cells are the resident immune cells. These large cells eat bacteria and debris that enter lobules. They are always touching these dangerous particles and exhibit a constant, low-level inflammation. Disruption of these cells can result in widespread, damaging liver inflammation. Finally, stellate cells store vitamin A, a critical vitamin. They are critical for promoting the liver’s amazing ability to regenerate. They form temporary scars that allow for healing. When they are damaged, however, they lose vitamin A. Damaged stellate cells can “activate” and run amok, secreting a lot of collagen that causes fibrosis and permanent scarring called cirrhosis. To understand the liver’s major functions, let’s first look at our body cells. Cells need to have a balance of chemicals to function properly. Normally cells control what goes in and out of them using special proteins. To keep unwanted things out, cells are separated from the environment around them. This separation is done by a membrane made of phospholipids. The –lipid at the end is another word for fat. Since the borders of our cells are made of fats, things that can pass through fats (called fat-soluble) can easily pass through the cell membranes. Cells can’t control this very well, so we use the liver instead. Let’s run through the liver’s major functions of storage, conversion, and creation. Storage is fairly simple. The liver stores fat-soluble vitamins and converts some of them into usable forms. It stores a quick supply of energy in the form of glycogen. Blood is stored in large quantities in the liver. This makes sense, because the liver is filtering the blood. Usually it holds a little more than 10% of the body’s blood, but the liver can expand to hold much more if needed. It can also squeeze blood out if the body is bleeding profusely. This probably isn’t great for the liver, but then again neither is bleeding out and dying. The liver converts a huge amount of material from one form into another. It acts as a gatekeeper for nearly all the blood in the body, including blood directly from the digestive tract. This includes tasty nutrients like fat and sugar, and dangerous toxins, like alcohol and methamphetamine. Blood is carried across the lobules and filtered through the hepatocytes and Kupffer cells. The liver doesn’t just remove dangerous particles, however, it metabolizes them! Metabolism is the conversion of chemicals from one form to another. One of the most important metabolic functions is detoxification. To make drugs and toxins less dangerous, the liver converts them from being fat-soluble (able to pass through cell membranes) to being water-soluble (able to be released through urine but much harder to enter cells). Carbohydrates are converted to glycogen for storage. The liver changes fats into energy for use. Proteins are broken into building blocks and waste products are removed. Remnants of dead blood cells called bilirubin are turned into bile and used for digestion. The conversion of materials into component parts helps the liver’s third broad function, creation. The liver creates, or synthesizes, many molecules that are used all around the body. It creates important hormones like angiotensin and thyroxine. It makes chemicals for the blood like prothrombin, fibrinogen, and clotting factors. It also makes the aforementioned bile, which is critical for digesting fats. The liver is the ultimate hero. Through all of these functions, the liver acts in the best interest of the body. It takes the hit from dangerous chemicals and sacrifices its own blood when we need it most. The liver is a team player of the highest degree. When it goes wrong we suffer throughout our whole body. Take care of that liver! Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Eng, F. J., & Friedman, S. L. (2000). Fibrogenesis I. New insights into hepatic stellate cell activation: the simple becomes complex. American Journal of Physiology-Gastrointestinal and Liver Physiology, 279(1), G7-G11. https://doi.org/10.1152/ajpgi.2000.279.1.G7 Geerts, A. (2001). History, heterogeneity, developmental biology, and functions of quiescent hepatic stellate cells. In Seminars in liver disease (Vol. 21, No. 03, pp. 311-336). https://doi.org/10.1055%2Fs-2001-17550 Kalra, A., Yetiskul, E., Wehrle, C. J., & Tuma, F. (2018). Physiology, liver. https://europepmc.org/article/nbk/nbk535438 Lautt, W. W. Hepatic Circulation: Physiology and Pathophysiology. San Rafael (CA): Morgan & Claypool Life Sciences; 2009. Chapter 2, Overview. https://www.ncbi.nlm.nih.gov/books/NBK53069/ Ozougwu, J. C. (2017). Physiology of the liver. International Journal of Research in Pharmacy and Biosciences, 4(8), 13-24. Vaja, R., & Rana, M. (2020). Drugs and the liver. Anaesthesia & Intensive Care Medicine, 21(10), 517-523. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7508170/ Yin, C., Evason, K. J., Asahina, K., & Stainier, D. Y. (2013). Hepatic stellate cells in liver development, regeneration, and cancer. The Journal of clinical investigation, 123(5), 1902-1910. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3635734/
Scroll down to listen to this article.
Listen to the article here:
The liver is an amazing and complex organ. It can regenerate from damage, helps us digest and function, filters some toxins, and in return gets thoroughly abused by us humans. Alcohol can damage the liver, but most livers are mistreated through other means, like diabetes and obesity. This is visible in the form of accumulated fat in the liver and can lead to serious problems. Nearly 1 in 4 adults in America have non-alcoholic fatty liver disease (NAFLD). When a fatty liver becomes inflamed and damaged it is called nonalcoholic steatohepatitis, or NASH. NASH is dangerous, and is an indication of decreased liver health. If untreated, NASH will degrade the liver, potentially leading to scarring known as fibrosis and permanent cirrhosis. Cirrhosis is cirrhiously bad. At this time, there are no approved therapies for the treatment of NASH. The current standard of care is exercise and weight loss to alleviate problems that damage the liver. Unfortunately, much like trying to lick your elbow, this is easier said than done. The consequences of an impaired liver include liver failure, cirrhosis, cancer, cardiovascular disease, and more. To alleviate this burden, scientists have identified several medical approaches to combating fatty liver. These approaches generally target the underlying mechanisms that lead to a fatty liver, aiming for a long-term solution. The broadest categories for investigative NASH medication are managing fat, sugar, and inflammation in the liver. One of the liver’s major jobs is to balance the body’s energy storage needs by managing fat. One method of dealing with excess fats is to dump extra fats out of the body through the digestive system. Thyroid hormone receptor beta (THR-β) can help us do just that. Receptors are parts of a cell that detect what’s happening outside its borders. They interact with hormones, sugars, fats, or other things. Each receptor only reacts to specific molecules. When activated, THR-β may help reduce the accumulation of fats in the liver by telling the body to move fats from the liver to the gut. Medications that activate THR-β are being investigated to see if they can also do this. Another method of helping the liver manage fat is to stop fats from being created in the first place. Unfortunately, some people create an unhealthy amount of fat. They may have a mutated gene called PNPLA3. PNPLA3 genetic disorder affects how the fat cells in the body deal with triglycerides. This mutation can increase liver fat and possibly lead to NASH. Scientists are working on ways of suppressing this gene. Other research targets being studied for limiting fat production include peroxisome proliferator-activated receptor alpha (PPARα). This is a chemical receptor on liver cells that regulates how fats are processed. When activated, this receptor can lower fat creation and lead to lower blood triglycerides (the most common type of fat). Rampant activation can be dangerous, however, so very specialized Selective PPARα Modulator (SPPARMα) medications are being developed to target the system with specificity and finesse. These medications also target and activate a very interesting hormone called fibroblast growth factor 21 (FGF21), which we will cover in the next section. Fats can’t take all the spotlight, though, because one of the biggest culprits of liver damage is actually sugar. As a cookie lover, this makes me very sad. Sugars, also called glucose, are converted into fats (stored in the liver) and can damage the liver, metabolic system, heart, etc. The body detects high levels of sugar in the pancreas. High blood sugar signals the release of insulin and amylin from the pancreas to the liver. The liver then starts breaking down, converting, and storing sugars. A couple of medications look to target this system to lower the burden on the liver and help with NASH. Fibroblast growth factor 21 (FGF21), mentioned above, has broad effects, including in the pancreas. It helps manage the body’s metabolism and homeostasis and makes the pancreas more sensitive to insulin. This may be particularly helpful for people with insulin resistance. Insulin resistance leads to type 2 diabetes. FGF21’s other effects appear to include increasing energy use, potentially leading to weight loss. Glucagon-like peptide-1 (GLP-1) agonists, like Semaglutide, Trulicity, and Mounjaro, act on the same system. These directly attach to pancreatic cells, preparing them for a large insulin release when they detect high glucose levels. It is hoped that this can help the liver deal with high blood sugar without taking damage. Another potential pathway to managing blood sugar is to send it down the yellow-brick road. Sodium-glucose cotransporter-2 (SGLT2) inhibitors deal with blood sugar by expelling it out of the body with urine. The final target of potential NASH treatments is inflammation. NASH stands for nonalcoholic steatohepatitis, which literally means “non-alcoholic inflammation of the liver (due to) fat.” Inflammation is like a visit with the inlaws: good when it doesn’t last too long. Researchers hope that reducing chronic inflammation may help limit the damage of NASH and prevent a worsening of the disease. Luckily, two avenues of treatment above also target inflammation. One complication of the PNPLA3 genetic mutation is an increase in cyclophilin, a protein that can increase inflammation. By reducing excess cyclophilin through PNPLA3 management – or by targeting it directly, inflammation may be relieved. Interestingly, FGF21, which may be used to lower blood sugar, appears to lower inflammation in the pancreas. The hope is that these medical interventions may also help the liver downstream. Overall, the liver is complex, and trying to keep it from being damaged is difficult. The only real treatment available today is weight loss through diet and exercise. With luck and help from the clinical trial process, there may be new avenues available in the future. Staff Writer / Editor Benton Lowey-Ball, BS, BFA
References: Fisher, F. M., & Maratos-Flier, E. (2016). Understanding the physiology of FGF21. Annual review of physiology, 78, 223-241. https://www.annualreviews.org/doi/full/10.1146/annurev-physiol-021115-105339 Geng, L., Lam, K. S., & Xu, A. (2020). The therapeutic potential of FGF21 in metabolic diseases: from bench to clinic. Nature Reviews Endocrinology, 16(11), 654-667. https://www.nature.com/articles/s41574-020-0386-0 Prasad, A. S. V. (2019). Biochemistry and molecular biology of mechanisms of action of fibrates–an overview. International Journal of Biochemistry Research & Review, 26(2), 1-12. https://doi.org/10.9734/ijbcrr/2019/v26i230094 Shen, J. H., Li, Y. L., Li, D., Wang, N. N., Jing, L., & Huang, Y. H. (2015). The rs738409 (I148M) variant of the PNPLA3 gene and cirrhosis: a meta-analysis. Journal of lipid research, 56(1), 167-175. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4274064/ Sinha, R. A., Bruinstroop, E., Singh, B. K., & Yen, P. M. (2019). Nonalcoholic fatty liver disease and hypercholesterolemia: roles of thyroid hormones, metabolites, and agonists. Thyroid, 29(9), 1173-1191. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6850905/ Ure, D. R., Trepanier, D. J., Mayo, P. R., & Foster, R. T. (2020). Cyclophilin inhibition as a potential treatment for nonalcoholic steatohepatitis (NASH). Expert opinion on investigational drugs, 29(2), 163-178. https://doi.org/10.1080/13543784.2020.1703948 US Department of Health and Human Services, National Institute of Health, National Institute of Diabetes and Digestive and Kidney Diseases. (April, 2021). Definition & facts of NAFLD & NASH. https://www.niddk.nih.gov/health-information/liver-disease/nafld-nash/definition-facts Wang, P., & Heitman, J. (2005). The cyclophilins. Genome biology, 6(7), 1-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1175980/
Scroll down to listen to this article.
Listen to the article here:
All diseases are different. Some are immediately apparent, like a heart attack. Some have the gall to hide undetected for years. This might sound nice, but the damage that can be done while undetected gets worse over time. Primary Biliary [billy-ur-ee] Cholangitis [kow-luhn-jai-tuhs] (PBC) destroys our bile ducts, often without our knowledge until other parts of the body are damaged. PBC is a somewhat rare disease, affecting 1 in every 3-4 thousand people, so around 100,000 Americans. Of these, around 90% of cases are in women. Most patients with PBC are diagnosed in their 50’s and 60’s, though the disease may start as young as 30. On its own, PBC may not have many symptoms, but leads to debilitating conditions of the liver such as cirrhosis, failure, and cancer. It also causes downstream damage across the body such as metabolic bone disease and malabsorption of nutrients. So what is Primary Biliary Cholangitis? There are clues in the name. The biliary system carries bile, a digestive fluid produced in the liver and sent to the gallbladder and intestines. Chol- also means bile, ang- means vessel, and -itis means inflamed. Cholangitis means the tubes that carry bile from the liver (called bile ducts) are inflamed. This disease is termed “primary” because it is the direct cause of inflammation and damage. A “secondary” disease is one caused by previous infection or disease; bile ducts can also be damaged by chemotherapy or surgical trauma to the lower bile system, for example. Altogether, primary biliary cholangitis is a disease that directly causes inflammation and damage to bile ducts. There are many bile ducts and many kinds of bile ducts, with the smallest being ultra-fine and located throughout the liver. These collect digestive fluid and transport them to ever bigger ducts to be stored in the gallbladder and sent to the digestive tract. In PBC, these small ducts are destroyed. A good rule of thumb is that when digestive fluid isn’t going to the digestive tract there may be problems. The buildup of bile damages the liver over time. Bile is critical for digesting fats and many vitamins. When bile fails to be de-livered to the digestive tract we may suffer malnutrition and fatigue. Most PBC patients are symptom-free but several experience debilitating symptoms, especially at later stages. Major symptoms are fatigue and itching (called pruritus). Jaundice, skin pigmentation, and fat buildup under the skin are other potential problems. Since so many people have no symptoms, or vague ones that can be attributed to other things, PBC is detected by looking at the blood. The primary evidence is the presence of antimitochondrial antibodies. These are immune system proteins that target mitochondria, the powerhouse of the cell. Increased antimitochondrial antibodies give us a good clue as to the true nature of primary biliary cholangitis. PBC is an autoimmune disorder – our immune system attacking healthy cells in the body. The cells at hand are the ones that make up the bile ducts. How this happens is complicated, and not fully known. We do know that there is a strong genetic component. X marks the spot in this case; since it affects mostly women, the X chromosome is a good candidate for where the trouble lies. The genetics aren’t enough, however. PBC requires an environmental component. Environmental in this case means anything that started outside of our own bodies and got in. Environmental risks include things that aren’t alive, like nail polish, hair dye, cigarettes, and toxic waste. Here at ENCORE Research Group we recommend avoiding toxic waste sites whenever possible. Living environmental factors include bacteria that degrade the immune system. This is a slow process. The bile duct cells become affected and some die. As they die they present parts of their mitochondria to the immune system, which learns to attack them. Eventually, the immune system starts attacking bile duct cells directly, causing scarring and cell death. This causes the eventual collapse of the small bile ducts. So what can be done? We can’t fight the underlying autoimmune disease yet. Current treatments are aimed at restoring the function of bile. The major medication is ursodeoxycholic [er-sudi-oxy-cholic] acid (UDCA), as synthetic bile acid. This only helps 60% of the time, and may be supplemented with obeticholic [oh-bet-i-colic] acid (OCA) to aid in the process. Neither of these help with symptoms. Itching may be treated with creams and cold water, and fatigue is treated with exercise, occupational, and physical therapy. Sicca, meaning dry eyes and mouth, is also a symptom, and is treated with artificial tears and saliva, or medications that increase these. Future treatments would target the underlying immune response or the associated inflammation. Either way, a treatment that stops damage is needed to help sufferers of PBC – and to keep those that aren’t suffering feeling well! Written By Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Dauphinee, J. A., & Sinclair, J. C. (1949). Primary biliary cirrhosis. Canadian Medical Association Journal, 61(1), 1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1591584/?page=1 Lleo, A., Invernizzi, P., Mackay, I. R., Prince, H., Zhong, R. Q., & Gershwin, M. E. (2008). Etiopathogenesis of primary biliary cirrhosis. World journal of gastroenterology: WJG, 14(21), 3328.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2716587/ Onofrio, F. Q., Hirschfield, G. M., & Gulamhusein, A. F. (2019). A practical review of primary biliary cholangitis for the gastroenterologist. Gastroenterology & hepatology, 15(3), 145. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6495411/ Ruemmele, P., Hofstaedter, F., & Gelbmann, C. M. (2009). Secondary sclerosing cholangitis. Nature Reviews Gastroenterology & Hepatology, 6(5), 287-295. https://www.nature.com/articles/nrgastro.2009.46 Strazzabosco, M., & Fabris, L. (2008). Functional anatomy of normal bile ducts. The Anatomical Record: Advances in Integrative Anatomy and Evolutionary Biology: Advances in Integrative Anatomy and Evolutionary Biology, 291(6), 653-660.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3743051/
Listen to the article here:
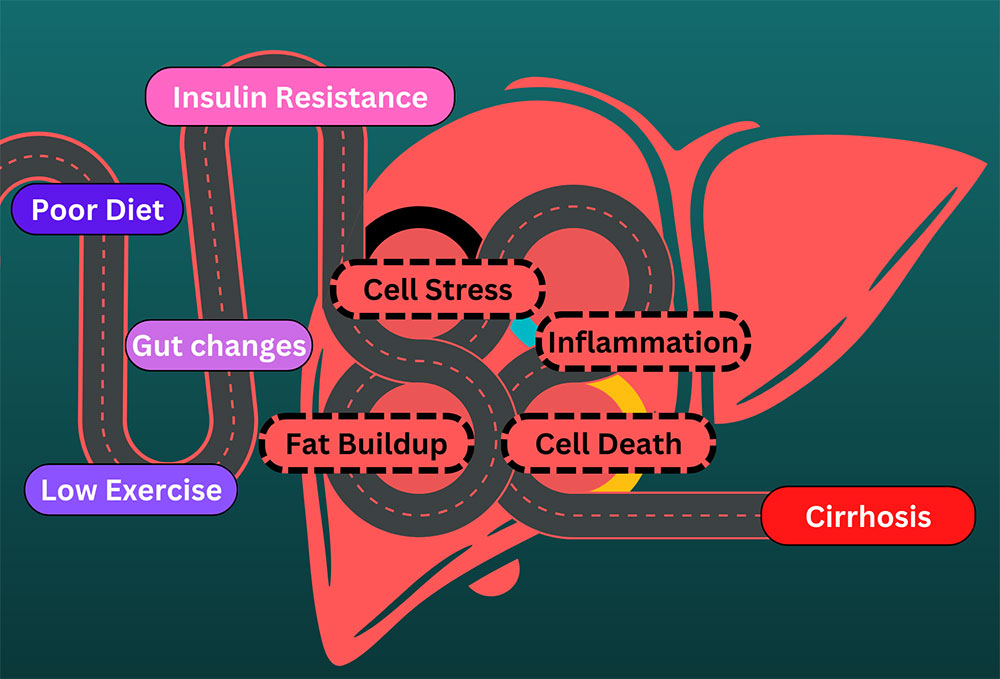
Fats are tasty in food, but not particularly good in the bloodstream. They can also be toxic to the liver and cells in general. We have special cells called adipose cells that store fat in our body. These cells have defenses against dangerous fat components called free fatty acids. Free fatty acids are the high-energy parts of fats, the part that gives you energy. Fatty acids are a great way to store energy and can be turned into power for your body, but the high energy content can also be dangerous in the wrong places. The liver transforms free fatty acids into usable energy. From here, the energy is delivered to cells all over the body. The liver is part of the system that makes sure the body’s energy demands match the available energy. Unfortunately, when too many free fatty acids are delivered to the liver, they can start to build up in the liver tissue and cause damage. Fatty liver is one of the most common ailments in Western countries. One in every three to four people in the US havw a fatty liver. Excessive alcohol consumption can cause a fatty liver, but most sufferers develop non-alcoholic fatty liver disease (NAFLD). Either way, people have steatosis. Steato- means fat, and -osis indicates a condition, especially an abnormal one. Steatosis of 5-10% is problematic and is the earliest indication that the liver is starting to suffer damage. Many people with fatty liver and no other abnormalities can make a full recovery, usually by stopping whatever is causing the steatosis. We know that alcohol can directly damage the liver, but how does NAFLD start? The causes are complicated, but some similarities exist. Excess fat released from fat cells, excess fat created by the liver, and excess fats from the diet all find their way into the liver. These are normally not an issue, but all are affected when the body isn’t regulating insulin properly. Insulin lets body parts know when you have food or are starving. When insulin isn’t processed correctly the body thinks it’s starving and tries to compensate – even when there is plenty of food present. In the middle of this the liver suffers. After a prolonged period of fat accumulation, a patient with NAFLD may develop non-alcoholic steatohepatitis, or NASH. Steato- for fat, hepat- indicating the liver, and -itis which means inflammation. This second leg on the terrible journey develops when fat causes inflammation in the liver. The gut changes and gives the wrong signals to the liver. Cells develop insulin resistance and can’t convert sugars into energy or fats correctly. Free fatty acids cause cell problems and elicit an immune response. Stresses on the liver cause a feedback loop, where inflammation disrupts cell function. The body tries to fix the liver but can’t overcome the massive amount of dangerous fats. Cells in the liver die, and the living cells can be damaged trying to compensate. With NASH, the inflammation is long-lasting, also called chronic. The liver can regenerate from NAFLD and NASH. It can’t sustain forever, however. When the liver is permanently damaged, the tissue can scar and die. This is a permanent reduction in liver function. We call this scarring Cirrhosis. Cirros- is the Greek word for yellow-brown (the color of a dying liver), and -osis refers to a condition, especially an abnormal one. Cirrhosis has multiple stages and can be asymptomatic but cannot be recovered from without intervention. The current treatment for cirrhosis is a liver transplant. Though we’ve been talking about the dangers of fats in the bloodstream and liver, it should be noted that the body makes a lot of these fats out of carbohydrates – sugars. A healthy diet without too many sugars and with lots of exercise are the best preventative measures for these conditions. Conditions related to insulin resistance, such as type 2 diabetes and metabolic syndrome can both cause and be caused by these conditions. Also, even though we have presented these as a pathway, note that you can progress from NASH to NAFLD or become symptom-free; it’s not a one-way journey! If you have any of these conditions, talk to your primary care physician to look for solutions. Also, keep an eye out for clinical research trials that may alleviate symptoms or the underlying fat buildup.
Sources: Pierantonelli, I., & Svegliati-Baroni, G. (2019). Nonalcoholic fatty liver disease: basic pathogenetic mechanisms in the progression from NAFLD to NASH. Transplantation, 103(1), e1-e13. . https://doi.org/10.1097/TP.0000000000002480 Sanyal, A. J. (2019). Past, present and future perspectives in nonalcoholic fatty liver disease. Nature reviews Gastroenterology & hepatology, 16(6), 377-386.
Listen to the article here:

The liver is an amazing and necessary organ. It can regenerate from a minor injury, break down dangerous chemicals and drugs, and help maintain the proper balance of nutrients, fats, and sugars in the body. It has hundreds of other important roles as well. With all this responsibility, we are in trouble when the liver stops working. One way the liver stops working is through non-alcoholic steatohepatitis (NASH). Steato- means fat, hepato- indicates the liver, and -itis means inflammation. Steatohepatitis is inflammation of the liver caused by fat accumulation. This is a progressive form of non-alcoholic fatty liver disease – the most common liver disorder in western countries. Progressive means that this disease gets more severe over time. NASH is a large problem in America, affecting 3-12% of adults. Furthermore, NASH can lead to cirrhosis, where the liver is permanently damaged, and lead to possible liver transplantation. Over a million adults in America have NASH-related cirrhosis. How do we get NASH? As the name indicates, this is not caused by alcohol. There are many pathways to developing NASH, but the underlying cause may be excess carbs and fatty acids. This can be due to diet or behavior, underlying genetics, or associated syndromes. Some of the syndromes associated with NASH are: The underlying mechanism of NASH can be very complex. A leading precursor to NASH is insulin resistance, where cells fail to respond to insulin. Conditions that cause or are caused by insulin resistance, such as type II diabetes and metabolic syndrome, may increase your chances of developing NASH. They also may develop or worsen as NASH symptoms get worse. Insulin resistance causes different types of fats to accumulate in the liver. This makes it very difficult for the liver to process the fats and they ultimately build up in liver cells. These fats, especially ones called nonesterified fatty acids (NFEAs), are very dangerous. They cause damage to liver cells and can also activate cytokines that start the inflammation process. Eventually, we get NASH, an inflammation cascade in the liver caused by fats. Cytokines start inflammation in the liver. Cell death attracts the immune system, which enters and causes inflammation while trying to help. Liver cells die and are less able to process fats, which leads to a compounding effect. Eventually, we may transition to cirrhosis, where permanent liver scarring and damage occur. There are few treatments on the market for NASH. As usual, the primary therapy for NASH is a good diet and regular exercise. Medicinal remedies are all in the experimental phases. Potential targets include increasing insulin sensitivity, decreasing fat creation, decreasing circulating fats, breaking fats down, and anti-inflammation treatments. One way to decrease circulating fats is by expelling them through the digestive system. In the liver, moving fats to the gut is regulated by thyroid hormones. Thyroid hormones activate receptors, which exist all over the body and cause many different effects. Thyroid hormone receptor Beta (THR-β) exists almost exclusively in the liver. Scientists are working to create medicines that activate THR-β and help clear fats from the liver in NASH patients. If you are interested in participating in a research study, contact your local ENCORE Research Group site today!
Sources: Noureddin, M., & Sanyal, A. J. (2018). Pathogenesis of NASH: the impact of multiple pathways. Current Hepatology Reports, 17, 350-360. Parthasarathy, G., Revelo, X., & Malhi, H. (2020). Pathogenesis of nonalcoholic steatohepatitis: an overview. Hepatology communications, 4(4), 478-492. https://doi.org/10.1002/hep4.1479 Pierantonelli, I., & Svegliati-Baroni, G. (2019). Nonalcoholic fatty liver disease: basic pathogenetic mechanisms in the progression from NAFLD to NASH. Transplantation, 103(1), e1-e13. . https://doi.org/10.1097/TP.0000000000002480 Pramfalk, C., Pedrelli, M., & Parini, P. (2011). Role of thyroid receptor β in lipid metabolism. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease, 1812(8), 929-937. https://doi.org/10.1016/j.bbadis.2010.12.019
Listen to the article here:

Celiac disease is a genetic autoimmune disease that affects the digestive system. It is triggered when a person consumes gluten, which is a protein found in rye, wheat, and barley. When a person with celiac disease eats gluten, their immune system reacts to the protein by attacking the small intestine. The role of the small intestine is to digest food and allow the body to use the nutrients. When the body attacks the small intestine, it damages the lining of the small intestine, resulting in symptoms that include bloating, abdominal pain, and weight loss. Eventually, after the small intestine has suffered damage, it can result in the body’s inability to absorb nutrients, therefore leading to a deficiency of nutrients and health problems. It is often difficult to tell if children have celiac disease, as the symptoms in children and adults differ. Symptoms in adults include: Adults can also experience a variety of symptoms unrelated to the digestive system, such as: Digestive problems are commonly seen in children with celiac disease, rather than in adults with celiac. Symptoms in children include: Symptoms are often not enough to tell if someone has celiac disease. People are more susceptible to celiac disease if they have some of the risk factors listed below: Diagnosis of celiac disease is through blood tests that check for certain antibodies and biomarkers. Often following these blood tests is an endoscopy/biopsy of the small intestine to evaluate the damage caused by the body’s response to the gluten protein. Although there is no cure for celiac disease, a change in diet helps to regulate the symptoms of celiac disease. A gluten-free diet often consists of gluten-free foods and vitamin and mineral supplements to regulate the body’s nutrients. Following a gluten-free diet allows the small intestine to heal. Doctors and dietitians can help guide people on their diet and inform them of gluten-free alternatives. This diet is normally life-long in order to prevent symptoms or a flare-up of the small intestine again. Doctors sometimes prescribe steroids as well to help regulate the inflammation of the small intestine. It is often difficult for people with celiac disease to eat out at restaurants or buy pre-made food from stores as it is tricky to be one hundred percent certain that a food is truly gluten-free. Stickers on foods say “may contain gluten” as a way to protect the manufacturing companies from lawsuits. However, most of the time the food does not contain gluten itself but has a small chance that it could have been cross-contaminated during the production process. This limits food that people with celiac disease feel safe consuming and buying. The FDA has standards that must be met in order for a food to be labeled as “gluten-free”. The final product must contain, at most, 20 mg/kg (20 parts per million) gluten or less. However, this rule does not apply to alcohol which can contain gluten. This amount of gluten (20 ppm) will not result in any side effects in a person with celiac disease, since it is too small of an amount. Another way people can be sure that they are consuming gluten-free foods is to call a restaurant ahead of time and ask if they have a gluten-free menu or serve alternatives for people with gluten intolerance. Written by: Sofia H. Davila, Clinical Researcher
Sources: Mayo Foundation for Medical Education and Research. (2021, August 10). Celiac disease. Mayo Clinic. Retrieved February 17, 2023, from https://www.mayoclinic.org/diseases-conditions/celiac-disease/diagnosis-treatment/drc-20352225 NCI Dictionary of Cancer terms. National Cancer Institute. (n.d.). Retrieved February 17, 2023, from https://www.cancer.gov/publications/dictionaries/cancer-terms/def/small-intestine U.S. Department of Health and Human Services. (n.d.). Eating, diet, & Nutrition for Celiac Disease. National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved February 20, 2023, from https://www.niddk.nih.gov/health-information/digestive-diseases/celiac-disease/eating-diet-nutrition
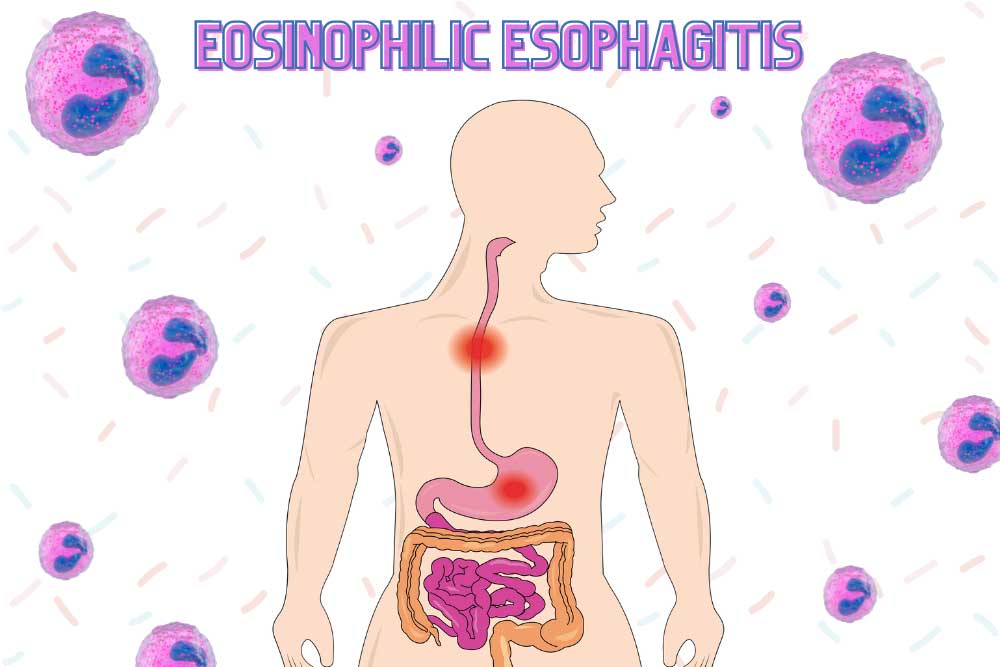
There are many ways to think of the human body. One of my favorites is that the body is like a donut. The inside of the donut is our entire body and everything that makes us what we are. The outside is our skin. The hole in the middle is made of our mouth, throat (esophagus), stomach, and intestines. The body treats the entirety of the digestive tract as the outside world. The intestines act like the skin; keeping most things out of the body and only letting specific molecules through. This has some important implications. The whole outside of the donut – including the throat and intestines – is covered in epithelial cells. These are tight cells that interact with the outside world. When these cells determine that they are touching something dangerous they signal to get rid of it immediately. This might feel like burning or itching on the skin, and may be something like diarrhea or vomiting in the digestive tract. These may feel crummy to us, but they are very useful in keeping us safe. The immune system is in charge of identifying and reacting to chemical and biological dangers. These can be harmful bacteria, worms, and things like splinters or some drugs. The immune system kicks into action, trying to kill or remove the dangerous particles without damaging body cells. This is a tricky dance. Antibodies will identify the dangerous particles or creatures and special B or T cells will widely sprinkle alarm particles, calling for reinforcements. What the body does next is determined by where the danger is found. In the gut – which the body treats as the dangerous outside world – the defenses are strong. One of the biggest guns we have is a cell called an eosinophil. These are very dangerous cells. They contain highly toxic particles and proteins that aggressively dunk in on invaders. They also signal to the intestines to contract and eject the contents. They only exist in specific parts of the body and are normally difficult to activate. Unfortunately, sometimes our body identifies otherwise safe items as dangerous. This is called allergies, and can be very annoying. Many of us suffer from seasonal allergies, but that doesn’t mean we should glaze over the dangers of allergic reactions. One difficult condition is eosinophilic esophagitis. Eosinophilic means it is caused by the dangerous eosinophil cells. Esophagitis refers to the fact that this happens in the esophagus, the throat. Eosinophils do not normally reside in the throat at all. The throat’s main job is to move food into the stomach, so it doesn’t need to detect danger. When eosinophils mistakenly reside in the throat, however, they can misidentify otherwise safe foods before the stomach gets a chance to digest them. This can result in the eosinophils damaging the throat. Eosinophilic esophagitis affects four in every thousand people, and can affect people of all ages. Most sufferers were diagnosed as children. In fact, it is one of the most common diagnoses for children who have trouble eating. It is chronic, or long lasting, and symptoms are debilitating. Sufferers experience inflammation of the throat, poor food intake, vomiting, and a poor appetite. Unfortunately there are few treatments available to fix this condition. The most effective has been reducing the diet of patients. This may consist of starting with a very strict diet and reincorporating food slowly to discover triggers. Scientists are actively looking at the underlying causes of why eosinophils are in the throat to begin with. Possible future treatments would likely stop eosinophils in the throat at a cellular or genetic level. The body may be a donut, but that doesn’t mean everything is tasty and fresh. If you are suffering from eosinophilic esophagitis or other conditions, call ENCORE Research Group and ask about studies you may qualify for. By Benton Lowey-Ball, BS Behavioral Neuroscience
Furuta, G. T., & Katzka, D. A. (2015). Eosinophilic esophagitis. New England Journal of Medicine, 373(17), 1640-1648. https://doi.org/10.1056%2FNEJMra1502863 Janeway Jr, C. A., Travers, P., Walport, M., & Shlomchik, M. J. (2001). Effector mechanisms in allergic reactions. In Immunobiology: The Immune System in Health and Disease. 5th edition. Garland Science. https://www.ncbi.nlm.nih.gov/books/NBK27112/ Rothenberg, M. E. (2004). Eosinophilic gastrointestinal disorders (EGID). Journal of Allergy and Clinical Immunology, 113(1), 11-28. https://doi.org/10.1016/j.jaci.2003.10.047 Zuo, L., & Rothenberg, M. E. (2007). Gastrointestinal eosinophilia. Immunology and allergy clinics of North America, 27(3), 443-455.https://doi.org/10.1016%2Fj.iac.2007.06.002
Listen to the article here:

Clostridioides difficile, C. difficile, or just C. diff is a particularly nasty bacteria that can make us very sick. The bacteria itself has the name difficile because it was difficult to isolate and study when it was first discovered. Forms of the problem bacteria are found all over the environment, but most can’t make us sick. The organism itself doesn’t kill cells like a virus; instead, it can produce toxins that can kill cells in the gut. C. diff has over 800 different strains, but only a few produce dangerous toxins. Overall, C. diff causes dangerous infections in hundreds of thousands of patients each year. Several people have C. diff inside their gut already, but it doesn’t cause them problems. Other bacteria in our gut can outcompete C. diff and keep it from causing damage. Unfortunately, one of the biggest medical breakthroughs, antibiotics, can destroy these helpful bacteria and allow C. diff to start running amok. In fact, any kind of immunosuppression can increase your risk of developing C. diff, including HIV/AIDS medications and those used after organ transplants. Being above 65 years old is another large risk factor. Close contact with some animals, like pigs, can also pose a risk. The most dangerous forms of C. diff are spread from person to person. This occurs with our most vulnerable populations: those in hospitals and those in elderly care. Due to the innate nature of care, people in hospitals and care homes can be exposed to C. diff unknowingly. How does C. diff survive in the notoriously clean hospital environment? The bacteria has a special trick up its sleeve; it can become dormant – and almost invincible. C. diff has two life cycle stages, the spore and vegetative stage. While in the spore stage, C. diff is inactive. It doesn’t need to eat or breathe. While in this stage it can survive in the environment, the stomach, through most antibiotics, and through alcohol washes. When a C. diff spore makes it into our gut, however, trouble can begin. It germinates in the duodenum – the part of the intestine connected to the stomach. Here it transforms into the vegetative stage. In the vegetative stage, C. diff is active. It can’t survive the stomach or in oxygen, but thrives in the intestines. Here it grows and reproduces. This is also where some strains produce dangerous toxins. The toxins of C. diff can produce a host of issues. The toxins can degrade and kill intestinal cells and cause inflammation of the intestines. Major symptoms are diarrhea, inflammation of the gut, and tissue necrosis (cell death). Other symptoms can include: So what can be done to fight C. diff? The first line of defense is the simplest: wash your hands! Prevention is the strongest barrier: avoid close contact with people who have an active infection and wash clothes and linens regularly. A medical professional (who should be wearing gloves!) can monitor any antibiotics an infected person is currently taking and might suggest probiotics. Some specific antibiotics target C. diff, including Metronidazole, Vancomycin, and Fidaxomicin. These may have unpleasant side effects, but can be effective. Treatments available include fecal microbiota transplantation (FMT), antitoxins, new antibiotics, and injectable antibodies. Additionally, prophylactics that can help protect the gut and vaccines against the dangerous toxins are in development. Keep an eye out, and with your participation in clinical trials, we can help protect those at the highest risk from C. diff! By Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Dayananda, P., & Wilcox, M. H. (2019). A review of mixed strain Clostridium difficile colonization and infection. Frontiers in microbiology, 10, 692.https://doi.org/10.3389/fmicb.2019.00692 Smits, W. K., Lyras, D., Lacy, D. B., Wilcox, M. H., & Kuijper, E. J. (2016). Clostridium difficile infection. Nature reviews Disease primers, 2(1), 1-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5453186/ U.S. Department of Health & Human Services/Centers for Disease Control and Prevention (September 7, 2022). What is C. diff https://www.cdc.gov/cdiff/what-is.html
Listen to the article here:
The liver is critical to maintain body function. Unfortunately, millions of Americans suffer from liver disease. When the liver suffers prolonged damage, scarring can form. This scarring, called cirrhosis, is debilitating and reduces liver function. Cirrhosis is sometimes called end stage liver disease, and is irreversible. On its own, cirrhosis can be painful and cause suffering, but is frequently made worse through complications. One of these is encephalopathy. Encephalopathy is a broad term used to describe several diseases and disorders. The unifying concept is that these diseases change the brain’s structure or function. When the cause of this change is through cirrhosis, the condition is called hepatic encephalopathy. This is the condition caused by cirrhosis of the liver, and can be horrible. It comes with a high mortality rate, over 25%, and affects over 30% of people with cirrhosis. The full mechanism of how hepatic encephalopathy works isn’t fully known. The most likely candidate for hepatic encephalopathy is a buildup of ammonia in the bloodstream. Ammonia is a common waste product for many cells. A damaged liver has trouble filtering ammonia from the blood. The ammonia accumulates in the blood where it can travel to the brain and cause confusion and disorientation at first. Additionally, liver damage can result in reduced muscle mass and immunosuppression. Muscles can remove excess ammonia from the blood, but may become damaged without a functional liver and be unable to help. A reduced immune system can lead to a buildup of harmful bacteria that produce excess ammonia. These combine to create excess toxic levels of ammonia in the bloodstream that make their way to the brain. The brain is normally protected from toxins in the blood through the blood brain barrier. Astrocytes are special cells in the brain that surround blood vessels and help filter the blood, letting only specific nutrients and particles through. Excess ammonia in the blood appears to damage astrocytes, with wide ranging effects on the brain. When the blood-brain barrier is reduced, toxins can enter the brain. This can lead to damage in neurotransmission, meaning the brain cannot function effectively. There is also an increased chance of infection in the brain and alterations to brain metabolism. This is a devastating compilation which can drastically reduce quality of life. In the early stages of hepatic encephalopathy, people may experience a general slowing of the brain. This is noticeable in attention, some motor response, and other vague areas. As the encephalopathy progresses, people experience more severe symptoms. Changes in personality have been reported, such as irritability and impulsivity. They may angrily buy m&ms in the checkout line. It also slows the brain and reduces its ability to function. People may become disoriented, experience distortions of time and space, become excessively sleepy, and descend into a coma. Clearly this condition needs medical attention! Luckily, hepatic encephalopathy can be reversible in many patients! The most important short-term treatment is to get rid of excess blood ammonia. The current standard of care is lactulose, a chemical that binds to ammonia and expels it rectally. This helps in the short term, and can also be recommended to help reduce recurrence. Though effective, lactulose is a laxative and can cause bloating, cramping, and other undesirable side effects. Because of this, many patients don’t like using this drug long term. Since the immune system is suppressed with cirrhosis, antibiotics may help as well. In fact, antibiotics may be helpful in preventing hepatic encephalopathy in the first place by eliminating harmful, ammonia producing bacteria before they can produce too much ammonia. Used with or without probiotics and drugs that help restore normal brain chemistry, we may be able to lower the burden of hepatic encephalopathy for those who suffer. Written by Benton Lowey-Ball, BS Behavioral Neuroscience
Sources: Bustamante, J., Rimola, A., Ventura, P. J., Navasa, M., Cirera, I., Reggiardo, V., & Rodés, J. (1999). Prognostic significance of hepatic encephalopathy in patients with cirrhosis. Journal of hepatology, 30(5), 890-895. https://doi.org/10.1016/s0168-8278(99)80144-5 Ferenci, P. (2017). Hepatic encephalopathy. Gastroenterology report, 5(2), 138-147. https://doi.org/10.1093/gastro/gox013
Listen to the article here:
Fatty liver disease is incredibly prevalent in the United States. Some estimates place the number of Americans with non-alcoholic fatty liver at over 30%, that’s around 100 million people in this country! Liver diseases are deadly serious; the liver is a critical organ and without it we cannot survive. The biggest problem with all liver diseases is that they frequently progress without symptoms. Because of this, the disease may progress to a dangerous or irreversible stage before it is even detected. Clearly, early, and routine testing for people at risk is critical. We can’t see the liver from the outside, so the only way to learn about how it is doing is by looking at it. We can look through the skin using technology or under a microscope using a biopsy. A biopsy – looking at a section of the liver under the microscope – is the “gold standard” of liver diagnostic techniques. This has drawbacks, however. Patients typically need to dedicate half a day to the procedure, and there can be rare complications. A biopsy is an invasive procedure requiring a piece of the liver be taken and examined. It is a critical piece of the liver diagnosis pie but is not a routine procedure to be done without cause. Imagining techniques can be very effective in diagnosing a fatty liver. Some techniques, such as a CAT scan and ultrasound, can’t diagnose the amount of scarring on the liver but can give an indication that there is fat present. CAT scans use x-rays, but imaging is otherwise safe. An ultrasound is fast and non-invasive. It is an excellent first step that many doctors use when they suspect a fatty liver. Magnetic Resonance Imaging (MRI) is the next best diagnostic procedure to a liver biopsy. With an MRI, doctors can clearly see the state of the liver. They are expensive, however. This again means they are an excellent tool for those who are known to have fatty liver but may not be an option for all patients to use regularly. Ultrasonic elastography is a different technique. It is commonly called Fibroscan, after the manufacturer of the diagnostic tool. Fibroscan uses sound waves to gently shake the liver and measure how it responds. The liver will stretch slightly. In a healthy liver, the tissue stretches more, but hard scar tissue is less elastic. The fibroscan can interpret the difference and determine how much fat and scar tissue is present. The test is very similar to an ultrasound; it is painless, fast, and safe. The fibroscan does not replace other imaging techniques but is cheap and effective at determining the stage of fatty liver present. Unlike other techniques, a Fibroscan can be done routinely for anyone who is at risk of having fatty liver. Fibroscans are very popular around the world, including in Europe, Asia, South America, and Canada. It is a cheap procedure with little reimbursement for practitioners, which unfortunately prevents widespread use in the USA. Risk factors for non-alcoholic fatty liver include being overweight or obese, being prediabetic or having diabetes, and eating a high-fat diet. If you are concerned about fatty liver, talk to your primary care physician and/or contact ENCORE Research Group for a complimentary Fibroscan. Written by Benton Lowey-Ball, BS Behavioral Neuroscience
Afdhal, N. H. (2012). Fibroscan (transient elastography) for the measurement of liver fibrosis. Gastroenterology & hepatology, 8(9), 605. Koren, M. (Host). (2022, July 20). Common fibroscan technology questions [Audio podcast episode]. In Medevidence! Truth behind the data. ENCORE Research Group. https://encoredocs.com/medevidence/ Koren, M. (Host). (2022, July 13). You cannot live without your liver [Audio podcast episode]. In Medevidence! Truth behind the data. ENCORE Research Group. https://encoredocs.com/medevidence
Listen to the article here:

Celiac disease is one of the major health issues on our planet, affecting around 1% of the population (that’s about 80 million people!). Celiac disease is more likely to occur in females. Though onset can occur at any age, it is most likely to be discovered around age two or during young adulthood. Celiac disease is commonly known as gluten intolerance and is classically characterized by its gastrointestinal symptoms including diarrhea, loss of appetite, weight loss, and other digestive issues. Additionally, there are other symptoms that are unrelated to the digestive system. These include anemia, bone density issues, neurological symptoms, skin rash, and more. Together these make for a severe detriment in the quality of life of most celiac sufferers. Like most autoimmune disorders, the leading symptoms come from the body’s immune system overreacting and causing damage. Celiac disease is unusual in that the reason for the immune response is gluten, which we eat. Gluten is a structural protein found in wheat, rye, barley, spelt, and kamut. Gluten isn’t fully digestible, and some intact protein pieces make it through the stomach into the intestines. In celiac patients, the protein pieces cross the intestinal lining and are mistaken for dangerous particles or microorganisms. This can trick the immune system into action, causing inflammation and damage. The number of people with celiac disease has been growing significantly. Five times as many people had the condition in 2000, compared with 1975. Scientists are still unsure why the disease has been growing worldwide. Better clinical testing, a spread of high gluten Mediterranean diets, and new varieties of grain are leading theories. Scientists have been able to discover much of the underlying mechanism of how celiac disease occurs, thankfully. It is genetic, and the key player appears to be HLA-DQ2 or HLA-DQ8 antigens which mistake gluten for danger. The presence of HLA-DQ2/DQ8 isn’t enough to guarantee celiac disease, but it is required. Additional contributors are thought to be other genes, environmental factors, and gut microbiota. Regardless, 95% of celiac patients have one of these dangerous antigens. Currently, the only treatment for celiac is a strict gluten-free diet. This can be difficult to maintain, and even with a gluten-free diet, some patients continue to have symptoms. Additionally, contaminants can be unknowingly present in food and even low amounts of gluten can cause a resurgence of symptoms. Scientists are looking for new ways to combat this disease and participating in clinical trials is the best way that you can help move celiac disease medicine forward. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Source: Caio, G., Volta, U., Sapone, A., Leffler, D. A., De Giorgio, R., Catassi, C., & Fasano, A. (2019). Celiac disease: a comprehensive current review. BMC medicine, 17(1), 1-20.
Listen to the article here:

Ulcerative colitis (UC) is a chronic and progressive autoimmune disorder that causes inflammation and ulcers to develop in the intestines, which can be very uncomfortable or debilitating. Ulcers are breaks or holes in the protective lining that can cause bloody diarrhea, with or without mucus. One of the significant symptoms of UC is a high urgency of bowel movements. Other symptoms include abdominal pain, bowel inflammation, and constipation. UC is not a fun condition to experience, to say the least! It is usually experienced in cycles of remission and relapse with periods of terrible high and thankfully low (or no) symptoms. The high periods can even lead to hospitalization. UC can develop at any age but is more likely to develop in people 15 to 30 years old. Interestingly, there seems to be a lower chance of developing UC if your appendix has been removed or if you are a smoker. This disease doesn’t play favorites, so there is no difference between men and women developing UC. Racial differences may be minimal compared to differences in diet and lifestyle. For example, a diet that includes eating refined sugars and processed grains may increase the likelihood of developing the disease. As mentioned above, diet can be a risk factor; this may be because of an immune response to the food. Research continues to show that the food you eat can affect all parts of the body. People with genetic factors have an immune system that attacks non-harmful gut bacteria, and low gut microbiota diversity may also be a risk factor. Ulcerative colitis often presents with other diseases. Data suggests that there is a relationship between UC and rheumatoid arthritis. Some experts think joint pain and swelling may be part of the same immune response responsible for ulcerative colitis. Other comorbidities include acute hepatitis (liver inflammation) and occasional skin conditions. Treatments for UC aim at inducing a period of remission. All of them come with side effects, so your doctors, specialist and primary care, should all be informed about the medications that you are taking. A particularly unpleasant and severe treatment is a colectomy or bowel resection, which removes part of the affected colon. 20-30% of people with UC may have to undergo this procedure. The good news is that researchers continue to look for better ways to treat UC. With your help, we can make a difference! Visit our enrolling studies page to get involved in the latest clinical research. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Sources: Gajendran, M., Loganathan, P., Jimenez, G., Catinella, A. P., Ng, N., Umapathy, C., … & Hashash, J. G. (2019). A comprehensive review and update on ulcerative colitis. Disease-a-month, 65(12), 100851. Lee, S. H., eun Kwon, J., & Cho, M. L. (2018). Immunological pathogenesis of inflammatory bowel disease. Intestinal research, 16(1), 26. Attalla MG, Singh SB, Khalid R, Umair M, Epenge E. Relationship between Ulcerative Colitis and Rheumatoid Arthritis: A Review. Cureus. 2019;11(9):e5695. Published 2019 Sep 18. doi:10.7759/cureus.5695
The liver is a critical organ that has many functions. It balances the body’s energy budget, filters blood, and metabolizes drugs, for a start. Since the liver is so imperative, it goes without saying that when the liver starts to fail, a lot can go wrong. It is widely known that excessive alcohol consumption can damage the liver, but there are also other pathways to liver damage. One particularly dangerous pathway for liver disease is Non-Alcoholic Steatohepatitis or NASH which is the most severe form of non-alcoholic fatty liver disease. The exact cause of NASH is unknown. NASH is a disease characterized by an accumulation of fat in the liver coupled with liver enlargement due to chronic inflammation and cell death. It is difficult to diagnose NASH. The symptoms, tiredness and/or pain in the upper right side of the abdomen, are not very specific to NASH or helpful in diagnosis. Most often, patients do not have symptoms at all until the later stages of the disease. NASH is widespread, affecting between 3-5% percent of the worldwide population. It has been referred to as a modern lifestyle disease, with things like overeating and sedentariness contributing to it. There are several risk factors for developing NASH: NASH is a progressive liver disease, meaning it gets worse over time without treatment or lifestyle changes. The first step of NASH is fibrosis, where repeated scarring occurs. This scarring forms when the liver is repeatedly damaged and healed. NASH patients develop more severe forms of fibrosis about twice as fast as those with alcohol-induced liver damage. In NASH, unlike with alcoholic liver disease, the cause of damage is not always known. Fibrosis is scarring that is reversible with treatment. If NASH progresses further, cirrhosis may occur. This is scarring and liver failure that is permanent, though people can live with it for years. In cirrhosis, the cells of the liver themselves suffer damage. The final two stages of NASH are hepatocellular carcinoma, a type of liver cancer, and death. Tackling NASH early on is vital to those suffering from this disease! Unfortunately NASH is an understudied disease with few routes to recovery. Currently, the most effective treatment appears to be weight loss, accompanied by dietary and lifestyle changes. In scientific studies, this has been only achievable by about 50% of those with NASH. With this in mind, and only the early fibrosis stage of NASH being reversible, the search for medications that can treat NASH has been described as the “Quest for the Holy Grail.” There are currently no FDA-approved drugs to treat NASH. Several clinical trials exist and will continue to enroll and may lead to a treatment soon. If you have NASH, it’s important to consider participating in clinical trials to help find effective treatments. Find out which clinical trials are enrolling near you by visiting our enrolling studies page. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Sources: Povsic, M., Wong, O. Y., Perry, R., & Bottomley, J. (2019). A structured literature review of the epidemiology and disease burden of non-alcoholic steatohepatitis (NASH). Advances in therapy, 36(7), 1574-1594. Sharma, M., Premkumar, M., Kulkarni, A. V., Kumar, P., Reddy, D. N., & Rao, N. P. (2021). Drugs for non-alcoholic steatohepatitis (NASH): quest for the holy grail. Journal of Clinical and Translational Hepatology, 9(1), 40.
Listen to the article here:

Chronic heartburn and acid reflux are symptoms of gastroesophageal reflux disease (GERD). This disease can result in the wearing away of the tube between the stomach and throat. When wearing away does not occur, a specific type of GERD occurs. This type is non-erosive reflux disease (NERD). The rates of GERD in the US are very large, affecting 1 in 5 people. Most of those cases are actually the NERD type. This works out to 14% of Americans experiencing NERD. It affects men and women at equal rates, and in the USA rates are constant across racial lines. Several factors can increase the chances of getting NERD. Your chances are increased with: NERD does not destroy the esophagus, but comes with its own host of issues. Heartburn and irritation of the food tube define NERD, and are uncomfortable on their own. It can also cause chest pain, vomiting, asthma, coughs, and sleeping problems. Furthermore, a major class of GERD-targeting drugs are less effective on the non-erosive form, NERD. These drugs are called proton-pump-inhibitors. Proton pump inhibitors are the most effective medications for treating GERD. Major name-brand proton-pump-inhibitors include Prilosec, Protonix, Nexium, Prevacid, and several others. The generic names are omeprazole, pantoprazole, esomeprazole, and others. All of these work by reducing the stomach’s ability to make stomach acid, lowering its ability to burn. As a result, GERD is both less painful and less destructive to the esophagus. Several people experiencing NERD are resistant to proton-pump-inhibitors. There are several possible reasons. In some patients, high concentrations of stomach acid isn’t the cause of their issues. In fact, only around half of NERD patients have abnormal acid levels, so lowering stomach acid may not be helpful as a treatment. These patients may have acid reflux even when acid levels are normal. They may also have a particularly sensitive esophagus. This could result in the feeling of heartburn even with lower acid levels. These patients need new treatments to help manage NERD. With luck, a clinical trial will pave the way to widespread adoption of an effective treatment soon!
Sources: Ang, D., How, C. H., & Ang, T. L. (2016). Persistent gastro-oesophageal reflux symptoms despite proton pump inhibitor therapy. Singapore medical journal, 57(10), 546. Dent, J., El-Serag, H. B., Wallander, M., & Johansson, S. (2005). Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut, 54(5), 710-717. Hershcovici, T., & Fass, R. (2010). Nonerosive reflux disease (NERD)-an update. Journal of neurogastroenterology and motility, 16(1), 8. ICRMD (2021, August 27). What is non-erosive reflux disease? ICRMD. Retrieved March 24, 2022, from https://icrmd.com/2021/08/27/what-is-non-erosive-reflux-disease/ Ribolsi, M., Cicala, M., Zentilin, P., Neri, M., Mauro, A., Efthymakis, K., … & Penagini, R. (2018). Prevalence and clinical characteristics of refractoriness to optimal proton pump inhibitor therapy in non‐erosive reflux disease. Alimentary Pharmacology & Therapeutics, 48(10), 1074-1081. Yamasaki, T., & Fass, R. (2017). Reflux hypersensitivity: a new functional esophageal disorder. Journal of Neurogastroenterology and Motility, 23(4), 495.
Listen to the article here:
Crohn’s disease is one of two types of irritable bowel disease. Unlike the more narrowly located Ulcerative Colitis, Crohn’s disease can be very widespread. Crohn’s disease is caused by inflammation of the bowel walls which can occur anywhere between the mouth and anus. This inflammation is frequently interspersed with healthy tissue. It affects the entire thickness of the bowel walls. Crohn’s is usually diagnosed by age 35 and affects 1.5 million people in the USA alone. Crohn’s disease is an autoimmune disorder. That means your body’s immune system is mistakenly attacking healthy cells. It is also a multifactorial disease. This means there are several possible underlying causes for it. Scientists know that the causes include genetic and environmental factors. Some risk factors are a low fiber diet, high carb diet, altered microbiome, and the use of NSAID medication. Lifestyle factors that influence Crohn’s include sleep, stress, exercise, and smoking. Unlike ulcerative colitis, smoking doubles a person’s chance of developing Crohn’s disease. Having such a large amount of possible causes makes Crohn’s disease very difficult to cure. So far researchers have only found ways to intermittently fix the symptoms of Crohn’s disease. Surgery has the best chance of providing long-term help however surgery comes with massive side effects. There are two classic drug-based solutions corticosteroids and immunomodulators. Corticosteroids reduce the body’s inflammatory response. Immunomodulators change how the immune system acts. The newest type of Crohn’s medication to market is biologics, which targets only specific parts of the immune system to keep effectiveness high and side effects low. Several of these are still in the research phase along with some brand new classes of oral drugs. To learn more about getting involved in Crohn’s disease research studies, visit our enrolling studies page or call your local ENCORE office today. Written by: Benton Lowey-Ball, B.S. Behavioral Neuroscience
Source Gajendran, M., Loganathan, P., Catinella, A. P., & Hashash, J. G. (2018). A comprehensive review and update on Crohn’s disease. Disease-a-month, 64(2), 20-57.
Listen to the article here:

Healthy eating and exercise can help with not only your waistline but also cardiometabolic health. Carrying around extra fat can negatively affect your whole body; some areas of concern include the liver, heart, and joints. Although many people can maintain a healthy diet and exercise routine to keep the weight off, some folks need extra help with medication.
The liver is the largest organ inside your body and is integral in filtering harmful substances from your blood. When too much fat builds up in your liver, this is called fatty liver disease. This can progress to damaging and scarring of the liver. The scaring can ultimately lead to liver failure. Lifestyle changes, like healthy eating and exercise, are currently the only treatments for fatty liver disease, although many clinical trials are currently looking for a safe and effective therapy.
Heart disease remains the world’s leading killer. While extra fat itself does not directly cause heart attacks, it leads to other causes that can. High cholesterol, high blood pressure, and diabetes are among those that build up plaque in the arteries leading to heart attacks. ENCORE Research Group offices have many clinical trials in these areas!
Being overweight can affect your joints by raising your risk of developing osteoarthritis. The extra weight puts additional stress on your weight-bearing joints, such as your knees, which can cause additional wear and tear. Additionally, inflammation associated with weight gain might contribute to problems in other joints such as the hands.
For the folks who need more than just a healthy diet and exercise to help with medical conditions, the good news is that many new cutting-edge treatments are being studied and are available to you. Call your local ENCORE Research Group office today to get involved in our research trials.
Sources:
heathline.com
health.clevelandclinic.org
health.harvard.edu

What is EoE? What are the symptoms? How to get diagnosed. Current research on EoE.
Eosinophilic esophagitis (EoE) is a chronic disease of the esophagus. Your esophagus is a muscular tube that carries food from your mouth to your stomach. EoE is when white blood cells (called eosinophils) build up in your esophagus.
Some of the most common symptoms of EoE are:
Your doctor will most likely want you to have an endoscopy to diagnose EoE. An endoscopy is a procedure where an endoscope (a tube with a light and camera attached at the end) is inserted into the body to let your doctor look inside an organ. For an esophageal endoscopy, the endoscope is put in your mouth and down your throat to examine the esophagus. But don’t worry, you’re not awake for that part! Other ways you can be diagnosed are biopsies, blood tests, and an esophageal sponge.
Science continues to move forward for new treatments of eosinophilic esophagitis, and we are delighted to be involved in these cutting-edge research trials at some of our ENCORE Research Group locations. To learn more about participating in our cutting-edge clinical trials, call our main office today! (904)-730-0166

A colonoscopy is used to detect any changes in the large intestine and rectum. A long flexible tube, called a colonoscope, is inserted into the rectum during the exam. At the end of the tube is a tiny video camera that allows the provider to view the inside of the colon. During the colonoscopy, your provider may also remove some abnormal tissue or take tissue samples if needed. It is common practice to receive a sedative before the exam to make you feel more comfortable, relaxed and decrease the chance of any pain. Both men and women need colonoscopies around the age of 50. If you are at a high risk for developing colorectal cancer, cancer that affects the colon and the rectum, your provider may ask you to receive a colonoscopy at an earlier age. You should reach out to your healthcare provider if you are having any symptoms of colorectal cancer because getting a colonoscopy could help prevent serious illness or even death. Symptoms include: There are many reasons why a colonoscopy is important. The main reason, as mentioned previously, is to test for colon cancer. Secondly, a colonoscopy investigates any problems with your intestines. If you are experiencing any abdominal pain or intestinal problems, let your doctor know beforehand. This way, your doctor can assess and find the answers to why you may be experiencing these issues. A colonoscopy also looks for abnormal tissues called polyps. A follow up colonoscopy might be necessary to remove all polyps to reduce your risk of colon cancer. Colon cancer is the third most common cancer among men and women over the age of 50. More clinical trials are needed in order to reduce this number and save lives. If you are in need of a colonoscopy, you may qualify for an enrolling study at one of our ENCORE Research Group locations. Participating in research trials have many benefits, including free medical attention, access to new technology and the chance to move medicine forward creating a healthier nation. Source: Borland Groover, American Cancer Society
What is a Colonoscopy?
Who Needs One and When?
Why are They Important?
Are there any Enrolling Studies at ENCORE Research Group?

The questions that have many people puzzled are finally going to be answered: What is gluten and is it actually bad for you? Gluten is a mixture of two types of proteins. It is responsible for the elastic texture of dough. These proteins are commonly found in wheat, rye, oats and barley. Gluten helps food keep its shape and acts like a glue that holds certain foods together. For those with celiac disease, gluten can be particularly dangerous. Gluten triggers an immune response in people with the disease, resulting in damages in the lining of the small intestine. These damages can obstruct a person’s ability to absorb nutrients from food and lead to problems like osteoporosis, infertility, nerve damage, and seizures. Adults with celiac disease show many digestive and other symptoms including: Digestive symptoms: Non-Digestive Symptoms: Gluten can be found in many different kinds of foods. It may be present in more foods than you think. The main foods to look out for which contain high amounts of gluten are processed foods, such as canned or boxed items, sweets, including cakes, pies and candies, cereals, bread, beer, pasta and more. Currently, the only treatment for celiac disease is to completely eradicate gluten from a person’s diet, which can be difficult. In order to help those suffering from this disease, it is imperative to do more research including participating in clinical trials. If you have celiac disease and want to be at the forefront of medicine, click the “enrolling studies” tab for more information about current clinical trials. Source: Harvard Health, Celiac Disease Foundation

What is H. pylori? H. pylori is short for helicobacter pylori, and it is a type of bacteria that grows in the stomach and can cause infection. This infection might be a lot more common than you think. With approximately 30-40% of the United States’ population containing the bacteria, there is no question as to how important more research needs to be done to combat it. If left untreated, H. pylori may cause peptic ulcers, gastritis, or stomach cancer. However, it often does not have any symptoms at all. What are the signs and symptoms? Many who contract H. pylori experience no symptoms at all, however when symptoms do occur, here is what you can expect: How do I get H. Pylori? Contracting H. pylori is common, and even more prevalent in developing countries. Some factors may increase your risk of infection like sharing a small, crowded living space, no access to clean water, and living with someone who has H. pylori. Some ways to reduce your risk of infection are to wash your hands before eating and after using the bathroom. Eat food that has been properly prepared and drink clean water. When should I see a doctor? As a good rule of thumb, you should always see a doctor if you have worsening stomach pains. You should also see a doctor if you have: Researchers are studying new ways to treat H. pylori infection and ENCORE Research Group is conducting some of these clinical trials. If you would like to help move research and medicine forward, visit our enrolling studies page to see clinical trials that are enrolling now in your area. Source: U.S. National Library on Medicine, Everyday Health, American Journal of Gastroenterology

Eosinophilic Esophagitis (EoE) is a chronic, immune-mediated disorder. It occurs in approximately 1 in 10,000 people and affects people of all age groups, with males being affected more frequently. EOE is associated with food allergies or other allergens, causing eosinophils (type of white blood cell) to migrate from the bone marrow (via blood) and settle in the esophagus causing inflammation to the esophagus. No one knows exactly why EoE occurs. People with EoE tend to have allergic conditions such asthma, seasonal allergies, allergic rhinitis, and eczema. Symptoms of EoE: EoE symptoms can overlap with symptoms of a condition called gastroesophageal reflux disease (GERD). Patients with EoE experience symptoms described as, If EoE is not controlled, the eosinophils will cause damage to the esophagus. Sometimes food that gets stuck in the esophagus (food impaction) may require emergency removal. How is EoE Diagnosed? If you have symptoms of EoE, your doctor will order a procedure called an endoscopy (EGD). An EGD is required to confirm the diagnosis and is performed by a specialist called a gastroenterologist. Patients are sedated for this procedure and a small flexible tube with a light and camera on the tip is inserted into the patient’s mouth. During the endoscopy, several biopsies of the esophagus will be taken and sent to the laboratory for analysis under a high-power microscope. EoE is confirmed when 15 or more eosinophils per high-power field are found (≥15 Eos/hpf). How is EoE Treated? Many patients with EoE are initially treated for GERD using a medication called a proton pump inhibitor (PPI). However, most EoE patients do no respond to anti-GERD treatment. Treatment with PPIs is given for a minimum of 8 weeks followed by a repeat EGD and biopsy. If the eosinophil count remains elevated (≥15/hpf), the diagnosis of EoE is confirmed and a different treatment is given. Patients with EoE are often referred to an allergy specialist for evaluation. Allergy testing can be done to identify which foods are triggering the EoE. Treatment for EoE usually includes dietary management and/or medication, or treatment on a clinical trial. If you have symptoms of EoE, it is important that you seek medical care and discuss your symptoms with your doctor. You can also learn more about EoE from advocacy organizations such as Apfed (apfed.org), or by joining an on-line patient communities such as Healtheo360 (healtheo360.com). Research is currently being conducted around the United States for this condition. Here at ENCORE Research Group we have 3 research sites with a new opportunity for people who have Eosinophilic Esophagitis. If you’re interested in learning more about this research, please contact your local research office below! Jacksonville: ENCORE Borland Groover Clinical Research 904-680-0872 Fleming Island Fleming Island Center for Clinical Research 904-621-0390 Inverness: Nature Coast Clinical Research 352-341-2100
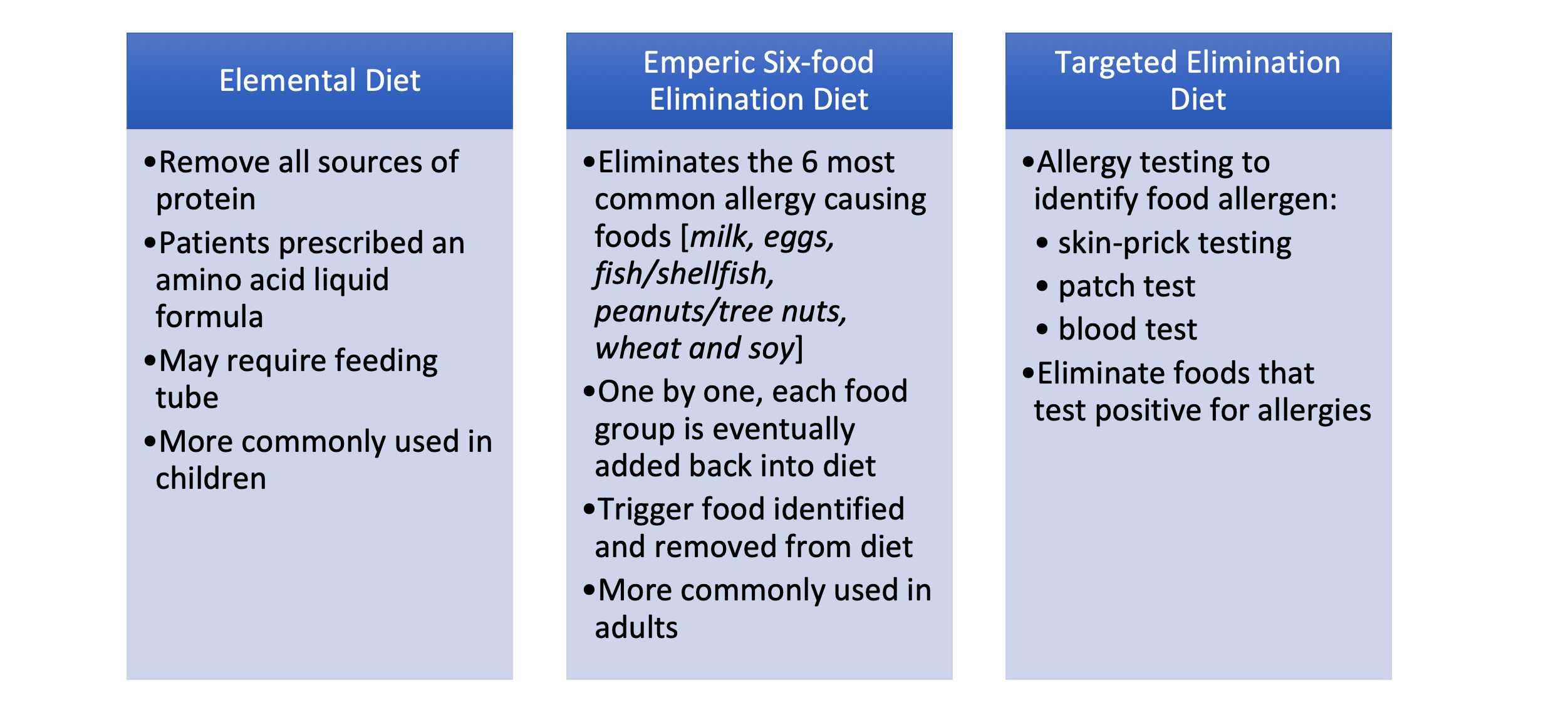


At some point in our lives we have all experienced acid reflux. Maybe it was after eating something spicy, or any acidic food like a tomato or certain dairy products and you felt a burning sensation in your throat. GERD, or gastroesophageal reflux disease is similar to acid reflux. GERD is a long-term condition where acid from your stomach overflows into the esophagus. If you experience acid reflux that occurs more than twice a week, your doctor may diagnose you with GERD. If you are experiencing these below symptoms more than twice a week, it may be time to see a doctor. Although GERD is a common condition affecting over 3 million Americans per year, if left untreated, it can lead to serious medical conditions. With certain lifestyle changes and medication, GERD can be treated. However, more research is needed to understand why there is a steady increase in Americans with GERD. Currently, ENCORE Research Group has enrolling studies for GERD taking place in Crystal River and Jacksonville. Visit our Enrolling Studies page to see what’s enrolling at a research site near you. Source: Medical News Today, Medline Plus
Ulcerative Colitis is a rare inflammatory bowel disease (IBD) with less than 200,000 cases per year. Ulcerative colitis can cause long-term effects on the body including inflammation and ulcers in the digestive tract. This can affect the innermost lining of the large intestine as well as the rectum. The symptoms of ulcerative colitis can range from mild to severe. Symptoms include rectal bleeding, bloody diarrhea, abdominal cramps and pain. Those who have Ulcerative Colitis are also at a greater risk of developing colon cancer. Doctors usually diagnose the different types of ulcerative colitis according to its location in the large intestine. The different types of ulcerative colitis include: Ulcerative Proctitis This is when the inflammation is in the area closest to the rectum. Rectal bleeding may be a sign of this disease, and it tends to be the mildest form. Proctosigmoiditis This type of ulcerative colitis is confined to the rectum as well as the lower end of the colon (sigmoid colon). Symptoms include abdominal cramps, bloody diarrhea, and the inability to move bowels, even though you feel as though you need to. Left-sided colitis If you have sharp pain on your left side, bloody diarrhea, abdominal cramping or weight loss, you may be experiencing left-sided colitis. This happens when inflammation extends from the rectum through the sigmoid and descending colon. Pancolitis Pancolitis often affects the entire colon. This can cause severe bloody diarrhea, abdominal cramps and pain, fatigue and weight loss. Acute severe ulcerative colitis This form of colitis is rare. It is a severe form and it affects the entire colon. It can cause severe pain, profuse bloody diarrhea, fever and complete loss of appetite. Although rare, ulcerative colitis can cause an abundance of health problems. It is imperative to participate in clinical trials in order to move medicine forward and help find effective treatments for ulcerative colitis sufferers. Resources: Cleveland Clinic, Crohn’s and Colitis
Crohn’s disease is a chronic irritable bowel disease (IBD). In those with crohn’s disease, an abnormal immune system causes chronic inflammation in the digestive tract. IBD affects nearly 3 million Americans, and there is still no known cure.
Symptoms of Crohn’s Disease
A person living with crohn’s disease can experience many symptoms and the severity can range from no pain at all to immobilizing. The symptoms include:
- Diarrhea
- Abdominal pain
- Cramping
- Weight Loss
- Blood in Stools
- Fatigue
- Nausea and vomiting
- No appetite
- Anemia
- Fever
Long-Term effects of Crohn’s Disease
Living with crohn’s disease can take its toll on the body long term. If left unmanaged, crohn’s disease can worsen and cause extreme pain and health concerns. Over time, crohn’s disease can cause severe damage to the GI tract. This can lead to:
- Fistulas. When excessive inflammation causes ulcers to form on the intestine, a fistula can form. A fistula is when two parts of the intestine connect to form a tunnel to drain the pus from the infected area.
- Intestinal Abscesses. This is caused by an excess of bacteria in the abdomen.
- Intestinal Blockages. This is a blockage that keeps food or liquid from passing through the small or large intestine. Symptoms can include severe abdominal pain, vomiting and inability to pass gas or stool.
- Internal Bleeding. This internal bleeding is caused by tears in the bowel wall due to inflammation in the colon. It is often the cause for diarrhea or bloody stool, a common symptom of crohn’s disease.
Crohn’s disease can be managed and those with the disease can live a very fulfilling life. The main goal of management is to treat the inflammation, which should reduce the severity of the symptoms and hopefully lead to long-term remission.
As mentioned, there is no known cure for crohn’s disease. The only way to find a cure and help those living with crohn’s disease is to participate in clinical trials to further research and hopefully, find a cure.
Resources: Centers for Disease Control and Prevention, Crohn’s and Colitis Foundation, Bladder and Bowel

Chronic pancreatitis is inflammation of the pancreas that does not heal but worsens over time. When you have chronic pancreatitis, your digestive enzymes begin to digest the pancreas itself. The pancreas is a small gland behind the stomach that secretes digestive juices into the small intestine. Eventually, chronic pancreatitis can damage a person’s digestive system and ability to make pancreatic hormones.
Some common causes of chronic pancreatitis are, but not limited to:
- Alcoholism
- Family history
- Autoimmune diseases
- A blocked pancreatic duct
- A genetic mutation such as mutations of the cystic fibrosis
Chronic pancreatitis, if unmanaged, can lead to:
- Diabetes- Chronic pancreatitis causes damage to the insulin-producing cells resulting in diabetes, a chronic condition where there is an abnormally high level of sugar in the blood.
- Pancreatic Cancer- If you have chronic pancreatitis, you are at an increased risk of developing pancreatic cancer by two to three
- Malnutrition- Chronic pancreatitis can cause your pancreas to produce fewer enzymes that are needed to break down and process nutrients from your Overtime, this may lead to malnutrition and significant weight loss.
Although there are many complications that may arise if you are living with chronic pancreatitis, the disease is treatable if caught in time. For chronic pancreatitis the treatments can be a hospital visit to treat dehydration, pain medication and a lifestyle change to a low-fat diet.
According to the type of pancreatitis that you have, other surgeries may be required.
One of the worst symptoms of pancreatitis is the severe abdominal pain. Currently, the only remedy for this is pain medication. In order to better understand and treat this pain more research needs to be done. The goal is to improve the quality of life and the risk of complications when living with pancreatitis.
Sources: MedlinePlus, Pancreatic Cancer Action, National Institute of Diabetes and Digestive and Kidney Diseases, National Pancreatitis foundation

More than just diarrhea…
Inflammatory Bowel Diseases include Crohn’s Disease and Ulcerative Colitis. These diseases cause inflammation in the digestive tract. Both diseases can have similar symptoms such as diarrhea, urgency, abdominal pain and cramping, fatigue, and rectal bleeding.
What’s the difference between Crohn’s and Ulcerative Colitis?
Crohn’s Disease can cause inflammation anywhere in the digestive tract, from the mouth to the anus. Ulcerative Colitis (UC) affects only the colon (also known as large intestine or large bowel). UC causes ulcers along with the inflammation and puts those affected at a higher risk of developing colon cancer.
What causes Ulcerative Colitis?
Physicians used to believe that stress and diet choices caused ulcerative colitis. Physicians now believe that UC was already present, and can be aggravated by these factors.
Research has shown that the immune system plays a role in developing Ulcerative Colitis.
My own immune system is giving me this disease?
There is no clear cause of UC. Medical science shows that an overactive immune system may be to blame. This can lead to continuous inflammation of the colon, and Ulcerative Colitis.
Many of the medicines currently prescribed to treat UC suppress (decrease the activity of) the immune system.
Is there a cure?
There is currently no medical cure for UC. Medical treatment is available to help manage it. American hospitals experience 500,000 visits per year and 46,000 hospitalizations for Ulcerative Colitis. In severe cases, surgical removal of the colon does cure ulcerative colitis.
The Good News
New medicines are now being studied with ENCORE Research to find a cure for UC. Please call for more information, or to schedule an evaluation to see if this is an option for you.
We look forward to talking with you!

Gastroenterology is the medical specialty concerned with the structure and function of the digestive tract (also called gastrointestinal [GI] tract). Some symptoms that can indicate disease or dysfunction of the GI tract include nausea, vomiting, weight loss, heartburn, regurgitation, abdominal pain, abdominal bloating, rectal bleeding, constipation, and diarrhea. Digestion of food and fluids is a very complex process, so persistent symptoms may require a gastroenterologist’s evaluation to determine the cause. Knowing the cause of symptoms can then lead to proper treatment and control or management.
What’s the Difference between IBS and IBD?
Irritable Bowel Syndrome (IBS)
IBS is a common GI disorder that can considerably reduce the quality of life. It affects as many as 5%-20% of individuals worldwide. It occurs more often in women than in men, and is more commonly diagnosed in patients younger than 50 years of age. Symptoms range from diarrhea to constipation, or a combination of the two. Abdominal pain or discomfort often exist alongside abdominal distension.
Diagnosis of IBS is made after obtaining a medical history, physical exam, and diagnostic testing to learn if any disease process is causing the symptoms. There is evidence to show that IBS can be a result of genetics, environment and social learning, dietary or intestinal microorganisms, low-grade inflammation and/or dysfunction of muscular movements, secretions and sensation.
Many patients with IBS ignore their symptoms, believing they are a normal part of everyday life. The good news is that with proper diagnosis, there are ways to treat or manage the symptoms. Don’t ignore persistent symptoms, there is help available.
Inflammatory Bowel Disease (IBD)
IBD is not the same as IBS, and understanding the difference is important for proper treatment. The symptoms can be the same, but the problem causing the symptoms is very different. Inflammatory bowel disease includes Crohn’s Disease (CD) and Ulcerative Colitis (UC). Crohn’s Disease can cause inflammation through the walls of the GI tract and can affect any part of the GI tract. Ulcerative Colitis commonly includes inflammation of the GI mucosa and is limited to the colon (large intestine). Recent research showed that some factors that can lead to IBD includes genetic susceptibility, environment, intestinal microorganisms, and immune responses. Medications are directed at treating the active inflammation, which can then decrease or control the symptoms.
Conclusion
Since symptoms of many GI disorders can be the same, a thorough medical history, physical exam, and proper diagnostic testing is crucial to obtaining a correct diagnosis and treatment. Open communication with your gastroenterologist and health care providers is essential to appropriate management and treatment. Be sure to tell your doctor about symptoms that concern you and new problems that arise. Do not hesitate to ask questions to ensure your understanding of your diagnosis and any treatment prescribed. Being a partner in your health care can lead to a healthier, happier life!
Written By: Julie Baker, RN
Resource: World Journal of Gastroenterology
Is GERD just heartburn, or is it something more? Check out our PowerPoint to find out the latest information and gain some tips on how to help reduce symptoms.
Researchers are continuing to study GERD and new ways to treat it. Currently, some of our ENCORE research sites have new GERD research studies enrolling. If you or someone you know has GERD, and are interested in participating, call your local office to find out more!
Click here to view the GERD powerpoint

Gluten Free. This has become a household term. Everyone has heard of gluten free diets, but not everyone comprehends why this distinction is necessary. For people with celiac disease, gluten can be devastating, and it is essential for food labeling to be correct. Celiac disease is an autoimmune disorder where the ingestion of gluten leads to damage in the small intestine. (1) Even ingesting minuscule quantities of gluten, such as crumbs from a toaster, can trigger intestinal damage. This damage can prevent the body from properly absorbing nutrients. Celiac disease is hereditary and is estimated to affect 1% of people worldwide.
There are more than 200 known symptoms of celiac disease, which can make it a nightmare to diagnose. It is estimated that there are 2.5 million undiagnosed Americans. When you mention celiac, most people think of digestive symptoms however, only around one-third of adults with the disorder experience digestive symptoms like diarrhea. Common symptoms include: fatigue, joint pain, arthritis, fatty liver, depression or anxiety, peripheral neuropathy, migraines, canker sores, and skin rash. If left untreated, Celiac disease can lead to many long-term health complications. Unfortunately, the only way to accurately diagnose celiac disease is to have an endoscopic biopsy. Once a diagnosis is made, the challenge of managing the condition begins.
Currently, the only effective treatment for celiac disease is to follow a strict gluten-free diet. However, the future is not bleak. Researchers from around the world are working to find effective pharmaceutical treatments. COUR Pharmaceuticals is researching a drug which aims to reprogram the body’s immune system to tolerate gluten subsequently reversing the signs and symptoms of Celiac disease.(2) Additionally, the Journal of Biological Chemistry notes that scientists have discovered a protein associated with celiac disease can be inactivated, paving the way for new treatment possibilities.(3)
References:
- https://celiac.org/celiac-disease/understanding-celiac-disease-2/what-is-celiac-disease/
- https://www.courpharma.com/pipeline-and-programs/
- https://www.sciencedaily.com/releases/2018/02/180223122343.htm

The liver is the second largest organ in the body. Its function is to process everything we eat or drink and filter out any harmful substances from the blood. When there is too much fat in one’s liver, the filtration process is interrupted and can become a health problem.
It is estimated that 25% of the world has Non-alcoholic Fatty Liver Disease (NAFLD), a precursor to NASH or Non-Alcoholic Steatohepatitis. NASH is associated with obesity, cardiovascular disease, type 2 diabetes and metabolic syndrome. It is now the most common liver disorder in the United States and the number one reason for liver transplants.
Starting as Fatty Liver Disease and then progressing to NASH, the buildup of fat in the liver can lead to inflammation of the liver and liver cell damage. Progression of NASH leads to fibrosis or stiffening of the liver and cirrhosis or scarring of the liver. NAFLD and NASH are both silent diseases with few symptoms even if the diseases progress to cirrhosis.
Physicians can monitor liver function blood tests as well as abdominal ultrasounds and liver Fibroscans to determine if you are at risk of developing NAFLD and NASH. However, the only way to definitely determine of you have NASH is to perform a liver biopsy.
The most common treatment for fatty liver disease is weight loss to reduce the fat in the liver. It is estimated that losing up to 3 to 5% of your body weight can help reduce the fat in the liver. Losing 10% of body weight may help reduce inflammation and even fibrosis in the liver. Currently, there are no medications which have been approved to treat fatty liver disease; however, many are in late stage development with promising results.
To learn more about current clinical trial opportunities for fatty liver disease and NASH, please contact us.

When patients are diagnosed with an autoimmune disorder they often have many questions. How did this happen? What is happening inside me? What treatments are available? Autoimmune diseases can be extremely complex and are the subject of much current research. The immune system’s purpose is to identify and destroy threats to the body such as viruses, bacteria or parasites. However, when a person has an autoimmune disease such as Crohn’s Disease, Lupus, Sjogren’s (show-grins) syndrome the immune system becomes unable to distinguish foreign bodies from the body’s own healthy tissue. When this happens, the immune system begins to target healthy cells causing inflammation. Almost any aspect of the immune system can malfunction causing a plethora of conditions.
One such condition is Crohn’s Disease. Crohn’s is an autoimmune disease where the immune system specifically targets the gastrointestinal tract. Crohn’s can be difficult to diagnose due to the variety of symptoms associated with the disease. The symptoms vary from person to person and by which component of the GI tract is being targeted. If a doctor suspects Crohn’s Disease, diagnosis is confirmed via an upper and/or lower endoscopy. Those living with Crohn’s disease will agree that we need to find a cure ASAP!
Systemic Lupus Erythematosus(SLE) is a chronic autoimmune disease in which the immune system can cause damaging inflammation to any part of the body. Skin, joints and organs can all be affected. Flares can cause a wide variety of symptoms. Around half of those affected by lupus have what is called a butterfly rash on their face. Other common symptoms include inflammation or swelling of the joints, and fatigue.
Another inflammatory autoimmune disease is Sjogren’s Syndrome. Sjogren’s is typically identified by its most prevalent symptoms, which are dry eyes and dry mouth. These symptoms occur because the immune system targets the glands that produce saliva.1 In the past treatment has almost entirely consisted of treating the symptoms of the disease. However, new research is showing that Sjogren’s can lead to other complications and scientists are now working on specially devised treatments to nip the problem in the bud!
According to JCCR’s Steven Mathews, MD “the last generation of autoimmune treatments worked further down the mountain so to speak and focused on treating the avalanche of symptoms. Current treatments are looking at treating conditions higher up the mountain at the source and preventing the avalanche from occurring.” Richard Smith, RN elaborated that, “general immunosuppressants act like a hammer on the immune system, whereas the current drugs we are researching act like a fine scalpel only targeting the rogue immune cells.” Our mission at ENCORE Research Group has always been to help get cutting edge treatments approved by the FDA. We want to help deliver safe and effective treatments to everyone. This is only possible by conducting research studies on new investigational medications. If you are interested in taking part in one of our research studies call today.
Growing up, we’ve all heard the saying, “An apple a day, keeps the doctor away” and in most cases, an apple is a great fruit to eat! However, if you have Crohn’s Disease that might not always be the case. Those afflicted with Crohn’s Disease actually have to peel the skin off of fruits and vegetables with edible skin, however delicious it may be! The skin is an insoluble fiber that can aggravate Crohn’s symptoms causing more gas, bloating, diarrhea and pain. In severe cases, can even cause blockages.
The cause of Crohn’s Disease is still unknown. Scientists believe the cause to be a mixture of environmental, and genetic factors. Crohn’s Disease causes inflammation of the wall of the gastrointestinal (GI) tract. The GI tract is continuous starting at the mouth and ending at the anus. An interesting fact about the GI tract is, it can be considered to be outside of the body. The body changes the environment of the GI tract to be conductive to digesting and absorbing food to the inside of the body. If we followed the journey of the apple discussed earlier after masticating and swallowing the apple is moved down the esophagus, and into the stomach where it will be digested. Next the apple will pass through a sphincter and into the small intestine where the nutrients from the apple will be absorbed. Crohn’s most commonly occurs in the small intestine and during a flare up it is difficult to absorb necessary nutrients before the bolus is moved to the large intestine.
While the small intestine is most commonly affected, with Crohn’s, any part of the GI tract explained above can be affected. The inflammation caused by Crohn’s produces flare ups and can lead to many uncomfortable symptoms. A few of which are: diarrhea, pain, unintentional weight loss, ulcers, malaise, anemia, and anal fissures.
Research has produced many significant advances for Crohn’s Disease, but there are still many unanswered questions. Our research sites are devoted to finding answers to those pressing questions and providing a better outlook for the future of Crohn’s health management. You can be an integral part of shaping the path for future medicine, by participating in a clinical trial.

Ask anyone who has had a Clostridium difficile (C. difficile, or C. diff) infection and they will probably tell you that it was one of the worst experiences of their life. Imagine the worst flu you’ve ever had but on steroids! C. diff is affectionately referred to as “deadly diarrhea” and with symptoms such as watery diarrhea 10 to 15 times a day that’s no joke! It can also come with a multitude of other symptoms such as: severe abdominal pain/cramping, rapid heart rate, fever, blood or pus in the stool, nausea, dehydration, and kidney failure.
What is C. Diff?
C. diff is one of the many different types of bacteria that lives in our intestines. It may sound gross but bacteria in your intestines are completely normal and you need a good balance of them to remain healthy. When something such as antibiotic use throws off the balance in your intestines C. diff may start to grow out of control and begin release toxins that attack the lining of the intestines which leads to that deadly diarrhea.
Is C. Diff contagious?
C. diff is contagious, so even if you were not recently on antibiotics, you can still catch C. diff by contact with a contaminated surface. Spores from C. diff bacteria come from human feces, soil, water and animal feces. These spores can also live for weeks or months outside the body.
Who is at risk?
C. diff is most often associated with doctor or healthcare facility visits or recent antibiotic use. There is a higher risk for adults ages 50 and over, especially those that have frequent doctor visits or have had any type of recent surgery or a hospitalization.
What can you do to lower your risk?
Good handwashing practices, especially after doctor or healthcare facility visits are a great start to lowering your risk of getting a C. diff infection. Another way is to take probiotics daily anytime you take an antibiotic. The reason for this is because when you take an antibiotic it not only kills off the bad bacteria, but it also kills off the good bacteria, giving C. diff a chance to thrive. Taking a probiotic, even if it’s just store bought yogurt, helps feed and rebalance your good gut bacteria. These are not fool proof, but they may help.
A Vaccine to prevent C. Diff?
While Handwashing and probiotics are certainly a must, researchers agree they are still not enough when it comes to preventing this life-threatening infection. Which is why we are involved in a cutting-edge research study working on the development of a new vaccine for C. diff prevention. If you are interested in volunteering, this study is for people ages 50 and up who have been recently hospitalized, have an upcoming surgery, or have frequent healthcare contact. If you are not sure if you qualify, please give our office a call or click below on the site that is closest to your location to sign up and we will be glad to answer any questions!
Fleming Island Center for Clinical Research
904-621-0390
Jacksonville Center for Clinical Research
904-730-0166